

 Print
Print facebook
facebook twitter
twitter Linkedin
Linkedin google+
google+

Introduction
A growing body of evidence suggests that contrast-enhanced ultrasound (CEUS) is a valuable, accurate, and cost-effective tool for characterizing focal hepatic lesions [1], often complementing indeterminate computed tomography (CT) and magnetic resonance imaging (MRI) results. CEUS can be a useful primary imaging tool for evaluating incidentally detected liver masses or liver masses in young patients and those with renal failure, allergies to contrast agents, or claustrophobia. Typical indications for CEUS for the characterization of focal liver lesions in non-cirrhotic and cirrhotic livers are summarized in the practice guidelines developed by joint World Federation for Ultrasound in Medicine and Biology (WFUMB) and European Federation of Societies for Ultrasound in Medicine and Biopsy (EFSUMB) initiatives [2].
Washout is an important imaging feature for characterizing liver masses and is often the initial step for differentiating liver masses when using a systematic diagnostic algorithm [3,4]. The presence of washout favors malignancy, whereas its absence suggests benignancy [4-6]. Metastases show more rapid washout [7] than hepatocellular carcinoma (HCC), in which the washout is often slow [8]. Washout in malignancy is more consistently demonstrated on CEUS than on CT/MRI due to the strictly intravascular property of the contrast agents [9]. Some malignancies with high vascular permeability and a large extracellular interstitial space, including intrahepatic cholangiocarcinoma (ICC), may fail to show washout on CT or MRI [10-14] due to leakage of the contrast agent through the vascular endothelium and accumulation in the tissue interstitium [9,15-18].
In this article, we briefly cover the typical timing of each vascular phase of CEUS and the properties of contrast agents, and explain the definition and types of washout on CEUS in accordance with the most recent (2017) version of the CEUS Liver Imaging Reporting and Data System (LI-RADS). We also explain the applications of these findings to the differential diagnosis of focal liver lesions with illustrative examples. In addition, we propose potential mechanisms of rapid washout in non-hepatocellular malignancies and describe the washout phenomenon in benign entities.
Contrast Agents and Scan Phases in CEUS
CEUS uses microbubble contrast agents that are gas-filled microspheres. The microbubbles are strictly intravascular because their size of several micrometers does not permit them to pass through the vascular endothelium into the interstitial space. Currently available second-generation CEUS contrast agents for liver imaging include SonoVue/Lumason (sulfur hexafluoride microbubbles, Bracco, Milano, Italy), and Definity/Luminity (perflutren lipid microspheres, Lantheus Medical Imaging, Billerica, MA, USA). Sonazoid (perfluorobutane, Daiichi-Sankyo, GE, Tokyo, Japan), which is actively used in Japan, South Korea, and Norway, enables additional liver evaluation in the Kupffer phase, as Sonazoid microbubbles are internalized by Kupffer cells. Sonazoid is not included in the 2017 version of the CEUS LI-RADS, although it is expected to be included in the next version of the CEUS LI-RADS.
The enhancement features at CEUS are documented along with the time units after injection of the contrast agent, expressed in seconds or minutes. Time zero is defined as the initiation of the saline flush [19]. The arterial phase starts at 10-20 seconds and lasts up to 30-45 seconds [2,19]. The portal venous phase starts at 30-45 seconds and lasts until 2 minutes [2,19]. The late phase lasts from the end of the portal venous phase until there is unequivocal clearance of microbubbles from the circulation at about 4-6 minutes [2,19].
Definition of Washout
Washout is defined by a visually assessed temporal reduction in enhancement in whole or in part relative to the composite liver tissue from an earlier to a later phase, resulting in hypoenhancement at any time, including the arterial phase, portal venous phase, and late phase [19]. The peak arterial phase enhancement before washout may be either in excess of (hyperenhancement) or equal to (isoenhancement) the enhancement of the adjacent parenchyma.
Significance of Washout in Differentiating Focal Liver Lesions
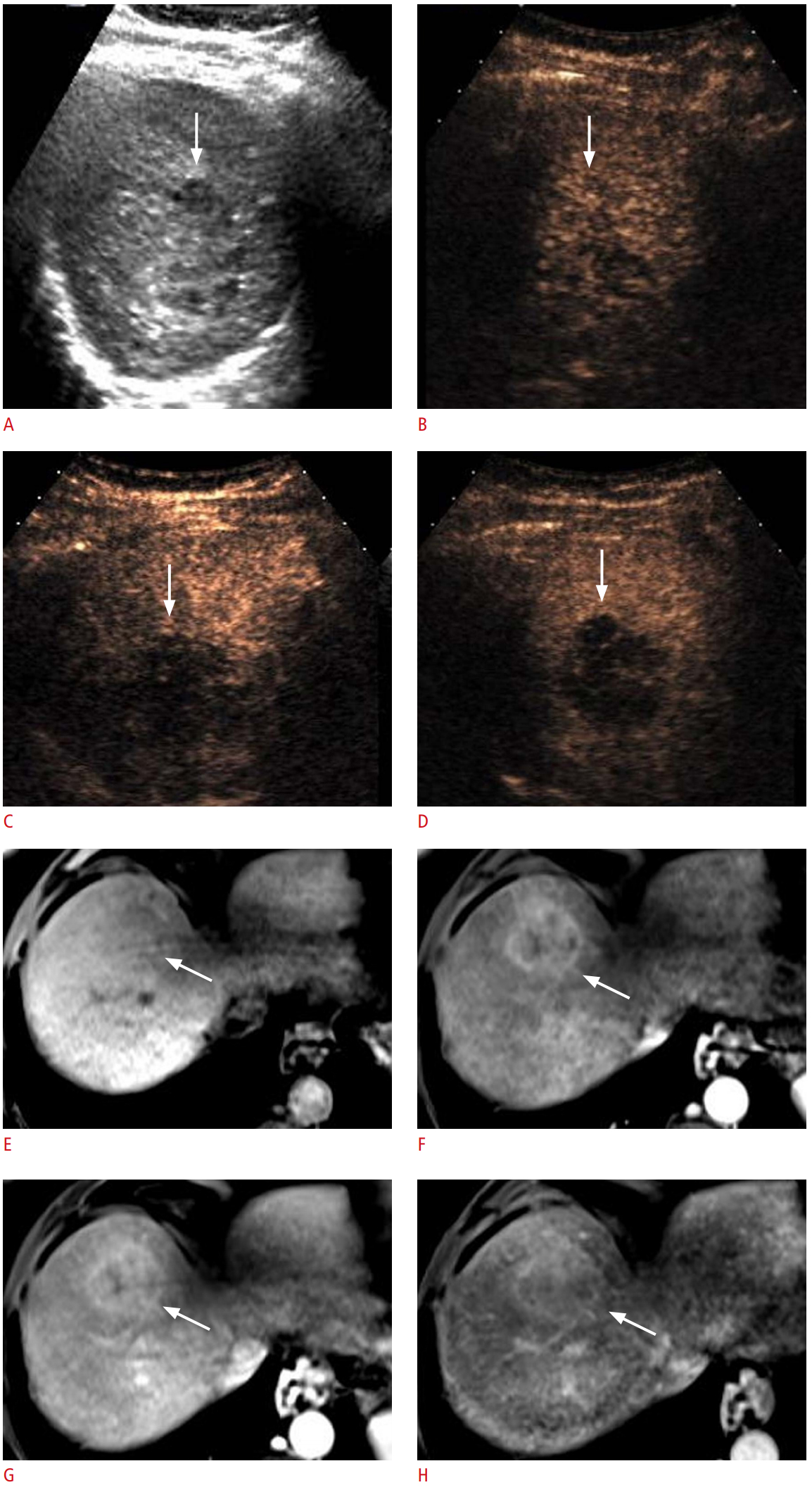
Evidence has shown that washout in the portal venous phase or late phase is the most important feature for distinguishing malignant lesions from benign lesions [4,20]. Therefore, it has been proposed to begin the algorithmic approach for diagnosing focal liver lesions on CEUS by evaluating the presence or absence of washout [4,21]. In a CEUS examination using a pure blood pool contrast agent, almost all malignant nodules, including ICC and other fibrotic tumors, show washout, reflecting the lower blood volume of malignant lesions relative to the liver. It should be noted that for ICC and other fibrotic tumors, there may be discordance in the presence of late-phase washout between CEUS and CT or MRI because the contrast materials used in CT and MRI can extravasate into the interstitium and accumulate progressively in the centrally located fibrous stroma, manifesting as late-phase hyperenhancement (Fig. 1) [22-24]. Understanding of this discordance is critical to reach the imaging diagnosis of ICC if present.
Infrequent exceptions to this algorithm have been reported for both benign and malignant masses on CEUS; in particular, some well-differentiated HCCs do not show washout [8], likely due to the similar blood volume of the lesion relative to the liver. Some benign liver masses, including hepatic adenomas, focal nodular hyperplasias (FNHs), and inflammatory pseudotumors may show washout [3,25,26]. It should also be noted that in patients with advanced cirrhosis, the presence and degree of washout of a focal liver lesion may be affected by poor enhancement of the background parenchyma due to decreased portal venous perfusion [27] and decreased vascular volume in the cirrhotic liver. In some cases of HCC, mild or no washout during the late phase can be partly attributed to the poorly enhancing hepatic parenchyma in the background. However, this may not be related to early washout in nonhepatocellular malignancies.
Characterizing Washout by Its Onset and Degree
In the 2017 version of CEUS LI-RADS, washout is categorized by its onset and degree (Table 1). Early washout is defined as washout that is unequivocally detectable earlier than 60 seconds after contrast injection [19]. Late washout refers to washout that is unequivocally detectable at 60 seconds or later [19]. Washout is considered mild when a nodule is hypoenhancing relative to the liver, but still shows substantial enhancement within 2 minutes after contrast injection [19]. Washout may appear marked at a later time (after 2 minutes), but if it becomes marked after 2 minutes, it is still characterized as mild. When washout occurs later than 2 minutes after contrast injection, the degree of washout is always mild. In contrast, marked washout occurs when a nodule appears almost black with minimal internal enhancement or is seen as a punched-out lesion within 2 minutes after contrast injection [19].
ICCs are occasionally found during HCC surveillance, although the incidence of ICC is much lower than that of HCC [28,29] and there are considerable differences between HCC and ICC in the treatment strategy and prognosis. Distinguishing between early and late washout and mild and marked washout is imperative for preventing misdiagnosis of ICC as HCC. The standard diagnostic hallmark of HCC on contrast imaging, consisting of arterial phase hyperenhancement (APHE) followed by the appearance of washout [30-34], is frequently seen on CEUS in cases of ICC in cirrhotic livers. However, subsequent studies have shown that the onset of washout occurs earlier in ICC than in HCC, mostly before 1 minute after contrast injection in ICC, and that the degree of washout is more marked in ICC than in HCC [35-39].
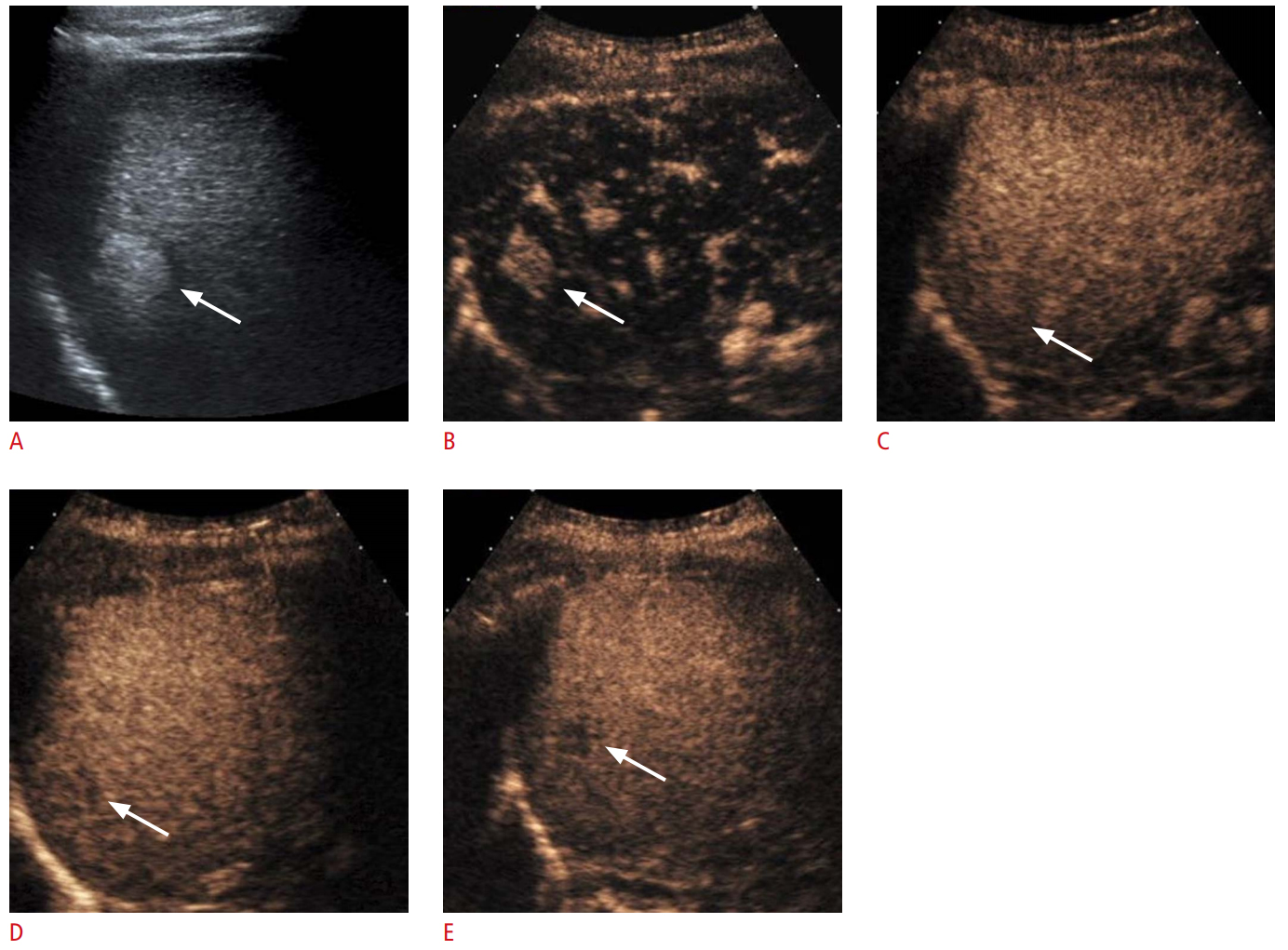
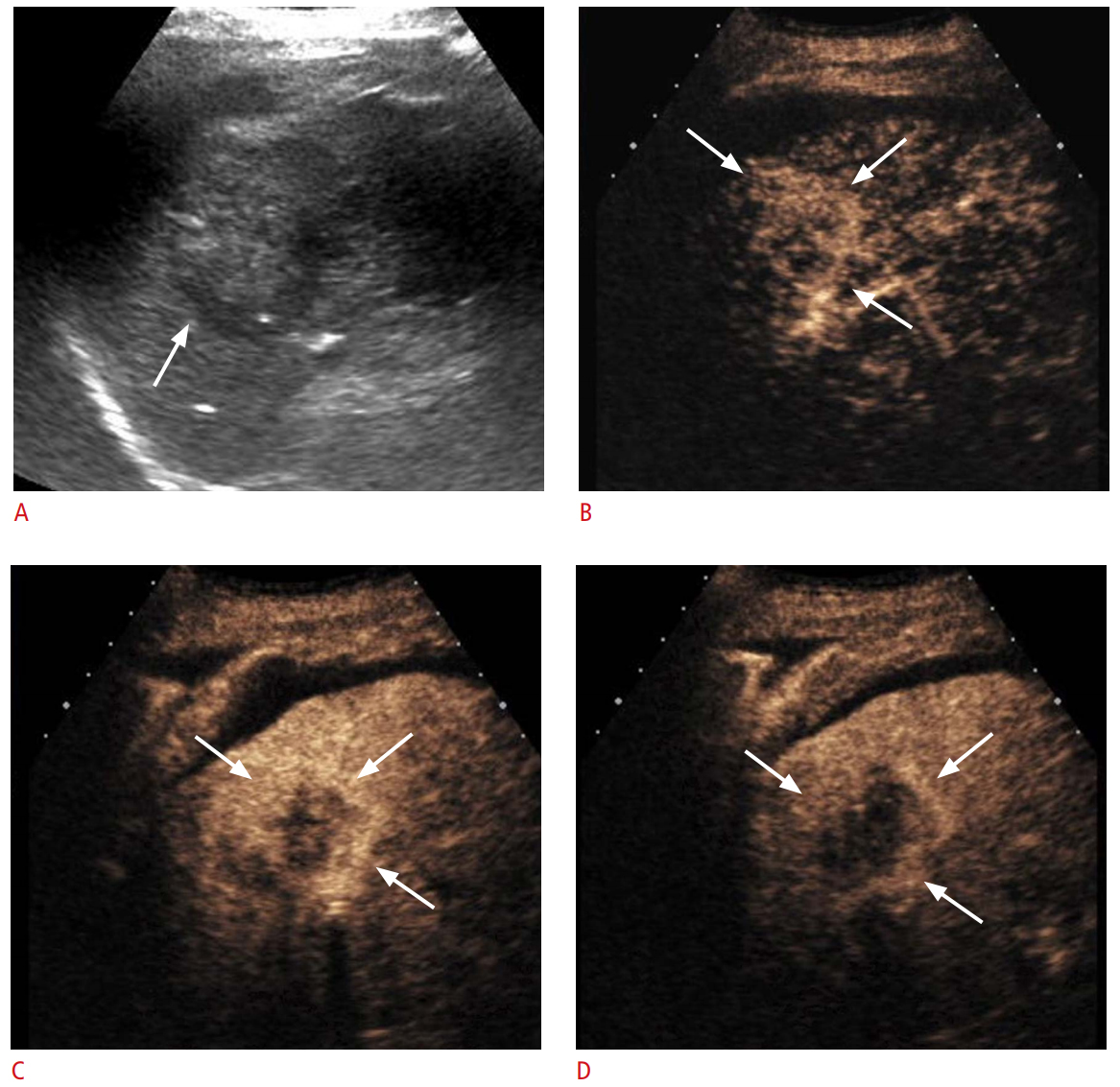
This information was reflected in the LR-5 and LR-M categories of the 2017 version of CEUS LI-RADS (Table 1). CEUS LI-RADS provides a diagnostic algorithm that categorizes observations in the liver from LR-1 (definitely benign) through LR-5 (definitely HCC) according to the observed size and enhancement pattern. The criteria for LR-5 are all of the following: APHE, a nodule size of ≥10 mm, and late and mild washout (Fig. 2). The APHE should show neither a rim nor a peripheral discontinuous globular pattern. The APHE is generally diffuse, although it may be partial. LR-M is assigned for lesions with imaging features that are probably or definitely malignant, but not HCC-specific. LR-M imaging features include rim APHE, early (<60 seconds) washout, or marked washout. If any one of those features exists in a lesion, LR-M is assigned. The differential diagnoses of LR-M observations include atypical HCCs and non-hepatocellular malignancies such as ICC (Fig. 3) and metastases (Fig. 4). With this updated scheme, in a recent retrospective study of 1,006 nodules from patients with chronic liver disease at risk of HCC, the LR-5 category was 98.5% (512 of 519) predictive of HCC, with no misdiagnosis of pure ICC as HCC [40]. If the 2005 American Association for the Study of Liver Diseases guidelines for CEUS (i.e., hyperenhancement in the arterial phase followed by washout in the portal venous phases regardless of its time of onset or intensity) [32] had been applied, the positive predictive value for HCC would have been 94% (512 of 580) [40], markedly lower than the current data of 98.5%.
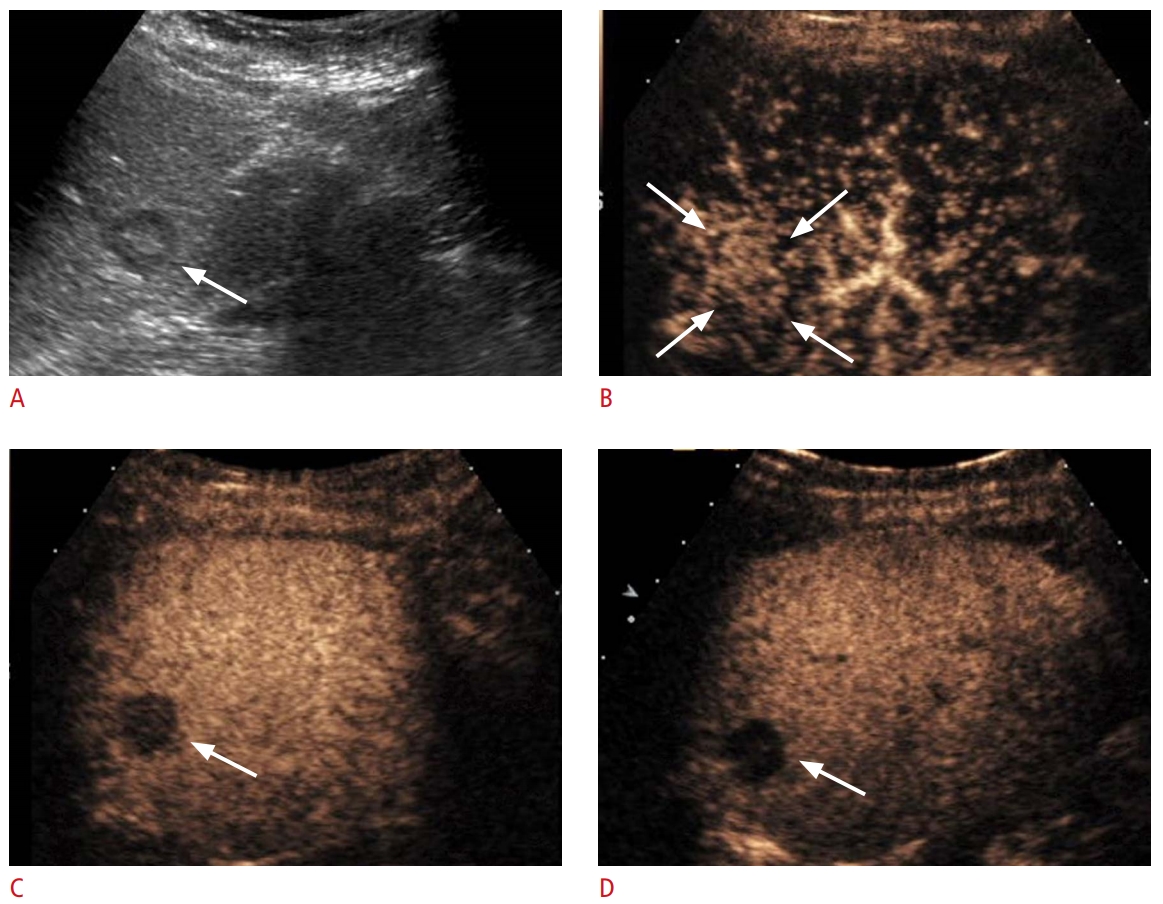
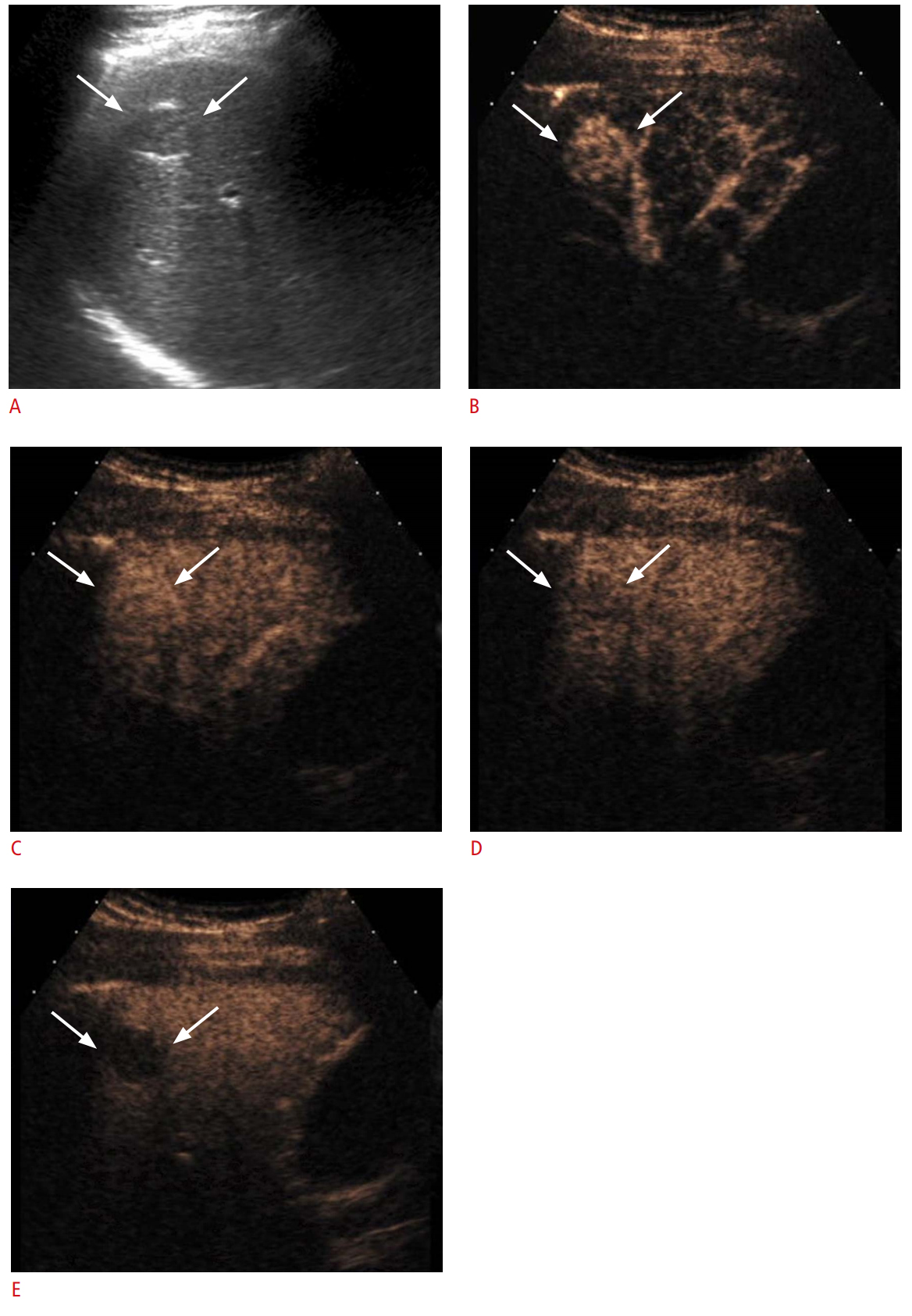
However, it should also be noted that a significant proportion of LR-M lesions on CEUS are HCCs, rather than non-hepatocellular malignancies. LR-M lesions usually require biopsy for diagnosis, in contrast to LR-5 lesions, which can be treated as HCC without further confirmation. A recent study demonstrated that 48% (39 of 82) of LR-M nodules on CEUS were HCCs, and the remainders were non-hepatocellular malignancies [40], in concordance with previous evidence revealing that a subset of HCCs showed early washout (Fig. 5) [41].
Potential Mechanisms of Rapid Washout in Non-hepatocellular Malignancies
Prior publications have shown that the tumor differentiation of HCC is related to the onset of washout, as more poorly differentiated HCC tends to show earlier washout [8,41,42]. Okamoto et al. [43] suggested that earlier washout in poorly differentiated trabeculartype HCC can be explained by the presence of fewer wide tumor sinusoids that allow faster blood flow, compared to HCCs of lower histological grades. In addition, a recent study reported that washout occurring at 10-30 seconds after injection of the contrast agent was a predictor of microvascular invasion in HCC, an expression of aggressive biological behavior [44]. Furthermore, earlier washout in non-hepatocellular malignancies (i.e., ICC or metastatic adenocarcinoma) than in HCC has been extensively reported [38,45-47]. Given those findings in the literature, it appears that the more distinct neoplastic cells are from normal hepatocytes in their nature, the more rapidly washout occurs.
However, the biological basis of the rapidity and degree of washout is not fully understood. Multiple contributory factors might exist, including early venous drainage from the lesion, lower vascular volume of the lesion relative to the liver, and persistent enhancement of the background liver. In patients with advanced cirrhosis, late and mild washout in HCC can also be partly explained by reduced enhancement of the cirrhotic liver parenchyma, presumably due to decreased portal venous perfusion [27] and decreased vascular volume.
Regarding the earlier and more marked washout of non-hepatocellular malignancies such as ICC or metastatic adenocarcinoma compared to HCC, we postulate that washout in the late phase mainly reflects the lower vascular volume of the liver lesion relative to the liver parenchyma. As the concentration of the microbubbles is uniformly distributed in the blood pool in the late phase, the degree of enhancement might depend mostly on the volume of the blood pool because the microbubble contrast agent for ultrasound is purely intravascular; thus, it is expected to be evenly distributed in the blood vessels. In a recent pilot study [48] that quantified the perfusion of hepatic lesions on CEUS, malignant lesions (HCC, ICC, metastases, and liposarcoma) showed significantly lower regional blood volume than benign lesions (FNH, adenoma, and hemangioma). In ICC and metastatic adenocarcinoma with desmoplastic reactions, fibrosis, and the absence of sinusoid-like structures, the vascular volume is particularly low.
Second, a previous study has proposed altered hemodynamics in hepatic metastases favoring early hepatic venous drainage, which may contribute to the rapid washout phenomenon. In patients with hepatic metastases, shorter arrival times and shorter times to peak in both the hepatic artery and hepatic vein, as well as a shorter hepatic artery to hepatic vein transit time, were noted on CEUS in comparison with normal volunteers [49]. These findings imply the presence of arterio-hepatic venous shunts in hepatic metastases, allowing the microbubbles to bypass the hepatic sinusoids. In contrast, Kitao et al. [50] reported that during multistep hepatocarcinogenesis, the drainage vessels of HCC changed from hepatic veins to hepatic sinusoids, and then to portal veins in the course of dedifferentiation. We suggest that these changes in the drainage vessels of HCC may be correlated to the changes in the washout onset of the nodules on CEUS. According to this proposal, when the drainage flows mainly into hepatic sinusoids and partially into the portal veins, late washout occurs. In the more advanced stage, when the portal veins become the main drainage vessels, washout occurs earlier.
Benign Entities Showing Washout: Potential Pitfalls
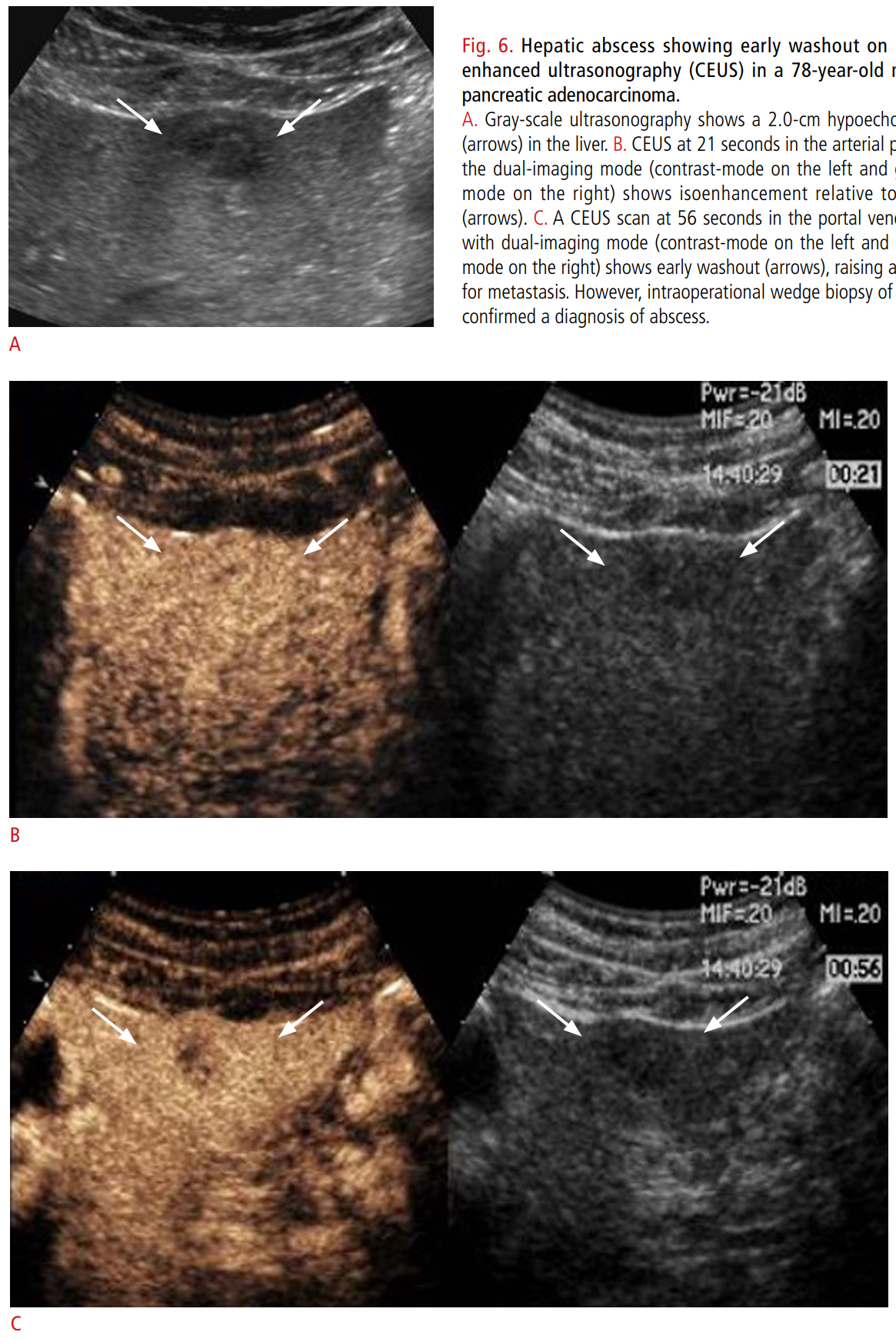
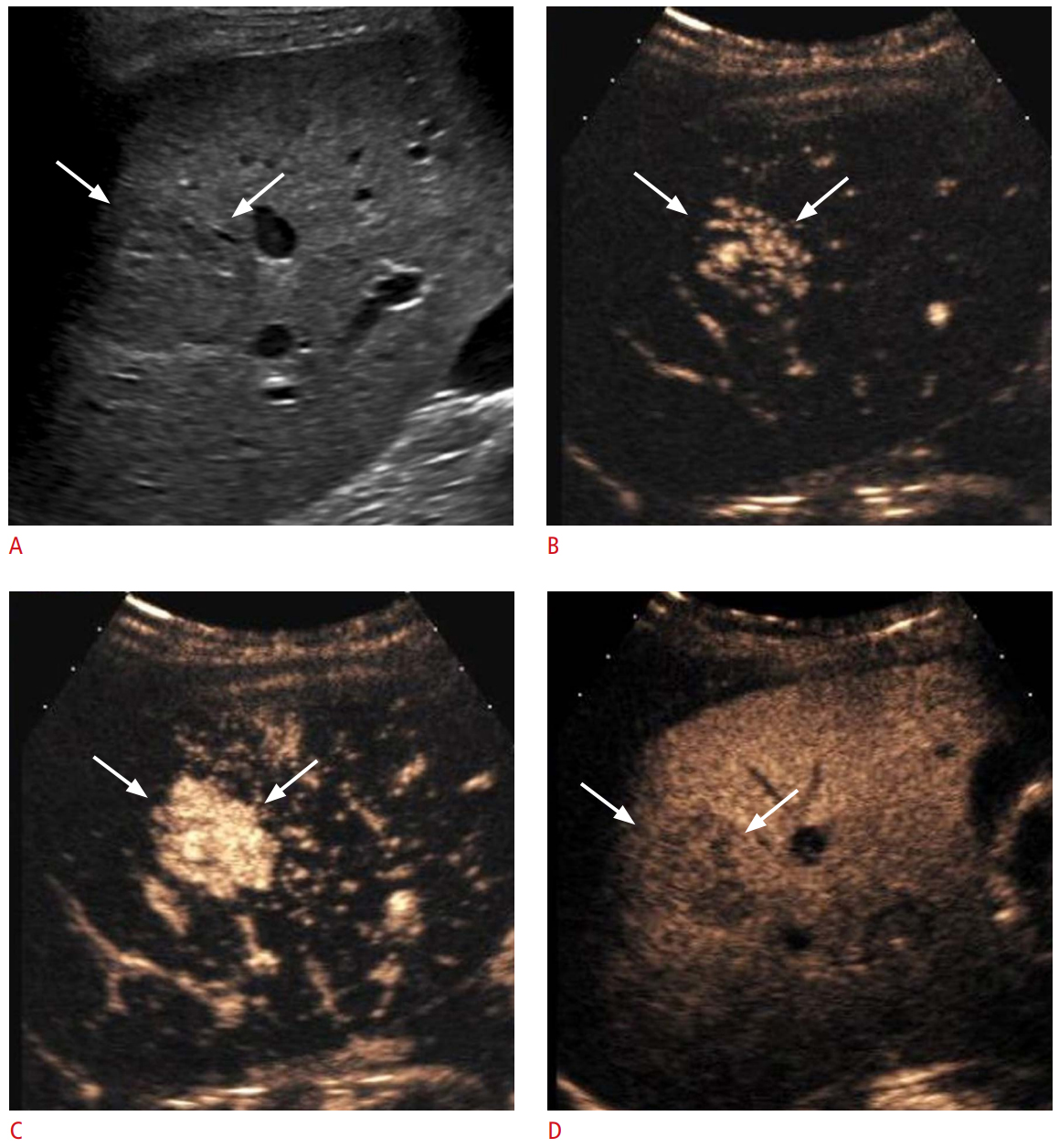
Although the washout phenomenon of malignant tumors in general is useful to differentiate them from benign lesions, some benign entities also infrequently show washout (Fig. 6) [3,25]. Washout has been reported in 0% to 14% of FNHs on CEUS depending on the study (Fig. 7) [25,51,52]. In the arterial phase, real-time assessment may demonstrate the characteristic spoke-wheel pattern of APHE with an inside-to-outside, or centrifugal, filling pattern [4] in typical cases of FNH. Studies have shown that some hepatocellular adenomas [25] and inflammatory pseudotumors [3,26] demonstrate washout. Adenomas often show APHE and demonstrate either sustained enhancement or mild washout in the late phase [25,53]. As approximately 30% of adenomas show mild washout in the late phase of CEUS [54,55], it may be difficult to differentiate adenoma from HCC. In such causes, the individual patient’s history of risk factors for HCC and demographics are important for differentiation, and a biopsy may be required in indeterminate cases. Insufficient data exist as to whether the presence and rapidity of washout on CEUS are related to the subtypes of hepatocellular adenomas. One study reported that two of six inflammatory adenomas and one of three HNF1a-inactivated adenomas showed late washout, while one of six inflammatory adenomas and one of three HNF1a-inactive adenomas showed washout beginning from the portal venous phase [54]. Inflammatory lesions such as immature abscesses may show early and marked washout, mimicking the enhancement pattern of non-hepatocellular malignant tumors [56,57]. They show APHE in both the center and the periphery of the nodule more frequently than rim APHE [57].
Conclusion
CEUS is a valuable and powerful tool for the evaluation of focal liver lesions. In the CEUS approach to the diagnosis of focal liver lesions, the presence or absence of washout is important for differentiating between malignant and benign lesions. The onset and degree of washout are useful for differentiating hepatocellular and non-hepatocellular malignancies. It is also important to recognize that benign liver lesions may infrequently show washout. Radiologists should be familiar with the definition and subtypes of washout and its potential pitfalls, as well as the concept that microbubbles are purely intravascular agents.
 Download Citation
Download Citation PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Full text via PMC
Full text via PMC



