

 Print
Print facebook
facebook twitter
twitter Linkedin
Linkedin google+
google+

Introduction
Inguinal hernia presents as a bulging mass over the groin area and accounts for 75% of abdominal wall hernias [1]. The reported lifetime risk of inguinal hernia is 27% in men and 3% in women [1]. The greater susceptibility of the male population is due to the persistent opening of the abdominal wall muscles for the passage of spermatic cords and testicular vessels. Inguinal hernias can be classified into direct and indirect hernias. Direct hernia is derived from protrusion of the intra-abdominal contents through a weak abdominal wall, while indirect hernia results from protrusion toward the inguinal canal. The prevalence of direct inguinal hernia is approximately half that of indirect inguinal hernia in the general population [1].
Ultrasonography (US) is the first modality of choice to examine palpable lesions at the inguinal area [2] due to its advantages, such as portability and an absence of radiation. Computed tomography (CT) and magnetic resonance imaging are regarded as problem-solving tools to be used after US. In older male patients, direct inguinal hernia with herniation of peritoneal fat is incidentally seen on abdominal and pelvic CT scans. US has been criticized for being operator-dependent, since a prompt diagnosis relies significantly on the examiner’s skill and experience. This review aims to provide an in-depth review of the use of US for the evaluation of inguinal hernia, with particular emphasis on the regional anatomy, relevant scanning tips, identification of subtypes, postoperative follow-up, and diagnosis of pathologies mimicking inguinal hernia.
Anatomy
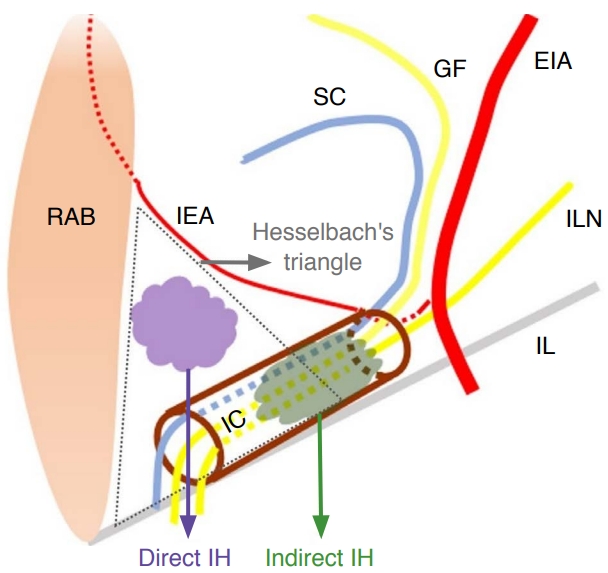
The inferior epigastric artery is an important landmark for differentiating direct inguinal hernia from the indirect subtype. It arises from the external iliac artery and travels posterior to the spermatic cord in men and posterior to the round ligament in women (Fig. 1) [3]. Subsequently, it ascends toward the midline, penetrates the transversalis fascia distal to the arcuate line, and enters the rectus sheath [4]. Above the arcuate line, the inferior epigastric artery travels between the posterior wall of the rectus abdominis muscle and the conjoint aponeurosis formed by the transverse abdominis muscle and the posterior half of the internal abdominal oblique muscle [4].
Notably, the inferior epigastric artery and Hesselbach’s ligament serve as the lateral border of Hesselbach’s triangle, the site of direct inguinal hernia (Fig. 1). Hesselbach’s ligament [4], also known as the interfoveolar ligament of Hesselbach, is a fibrous band emerging from the inferior border of the transversalis fascia, which attaches to the superior pubic ramus. The medial margin of the triangle includes the lateral edge of the rectus abdominis muscle and the ligament of Henle [4]. The latter term has been used interchangeably with the conjoint tendon or the inguinal aponeurotic falx in certain studies. It is derived from conjunction of the fasciae of the internal abdominal oblique and transverse abdominis muscles [4]. The inguinal ligament, which bridges the anterior superior iliac spine and the pubic tubercle, forms the inferior border of Hesselbach’s triangle. It also constitutes the floor of the inguinal canal [5].
Abdominal contents sliding through the inguinal canal elicit indirect inguinal hernia (Fig. 1) [1]. The anterior wall of the inguinal canal is derived from the aponeurosis of the external and internal abdominal oblique muscles, whereas the transversalis fascia serves as the posterior wall of the inguinal canal [6]. The roof of the inguinal canal is formed by the internal oblique and transverse abdominis muscles, while the inguinal and lacunar ligaments constitute the floor [6]. The lacunar ligament is the medial extension of the inguinal ligament and originates from the inferior border of the aponeurosis of the external abdominal oblique muscle [4]. There are two openings in the inguinal canal: the superficial and deep inguinal rings. The deep inguinal ring is an aperture on the transversalis fascia and is located cranial to the inguinal ligament and lateral to the inferior epigastric artery. The superficial inguinal ring is a triangular orifice over the aponeurosis of the external abdominal oblique muscle and is positioned cranial/lateral to the pubic tubercle. The inguinal canal harbors the ilioinguinal nerve, the genital branch of the genitofemoral nerve, the spermatic cord in men, and the round ligament in women.
Ultrasonographic Anatomy
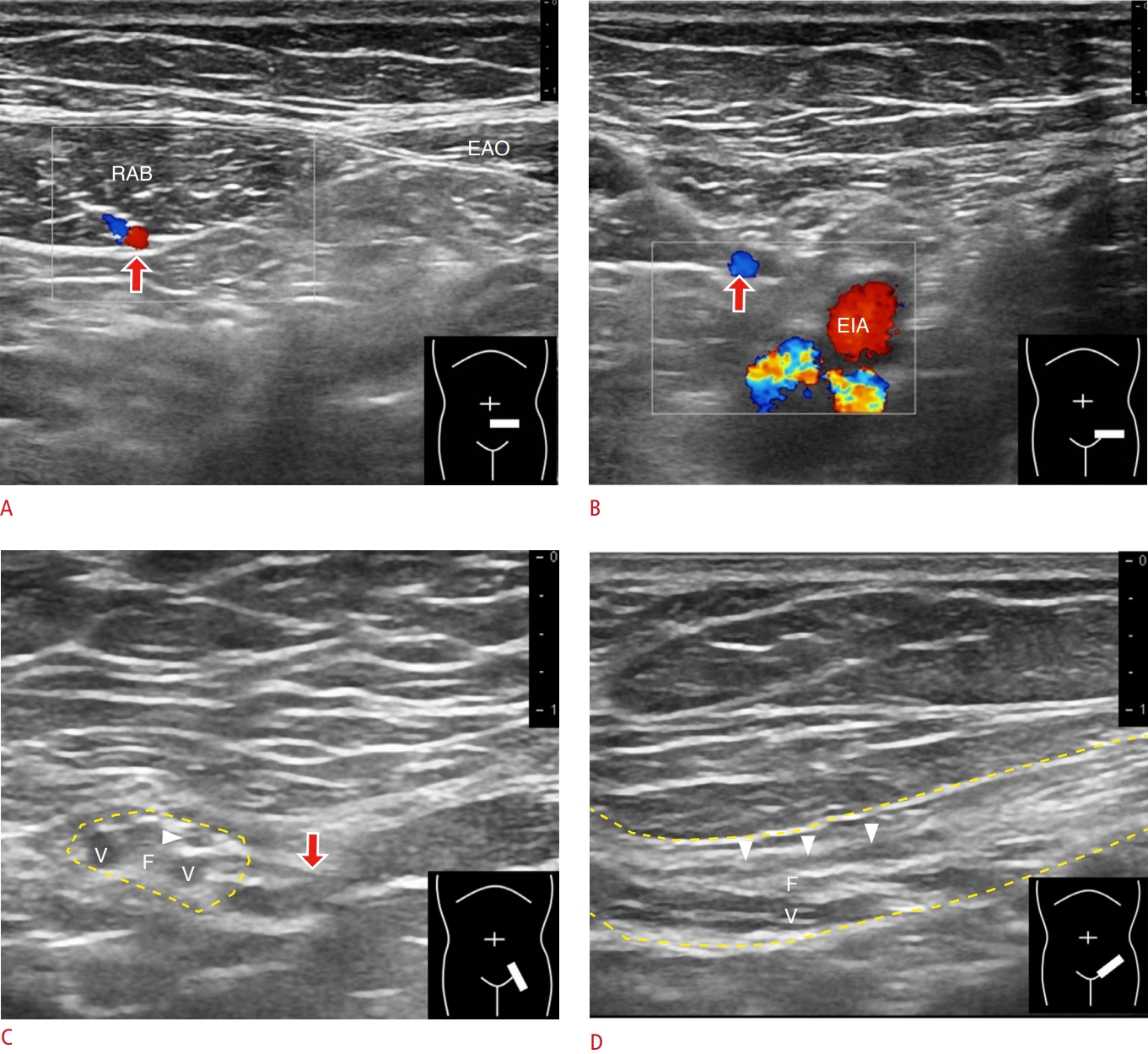
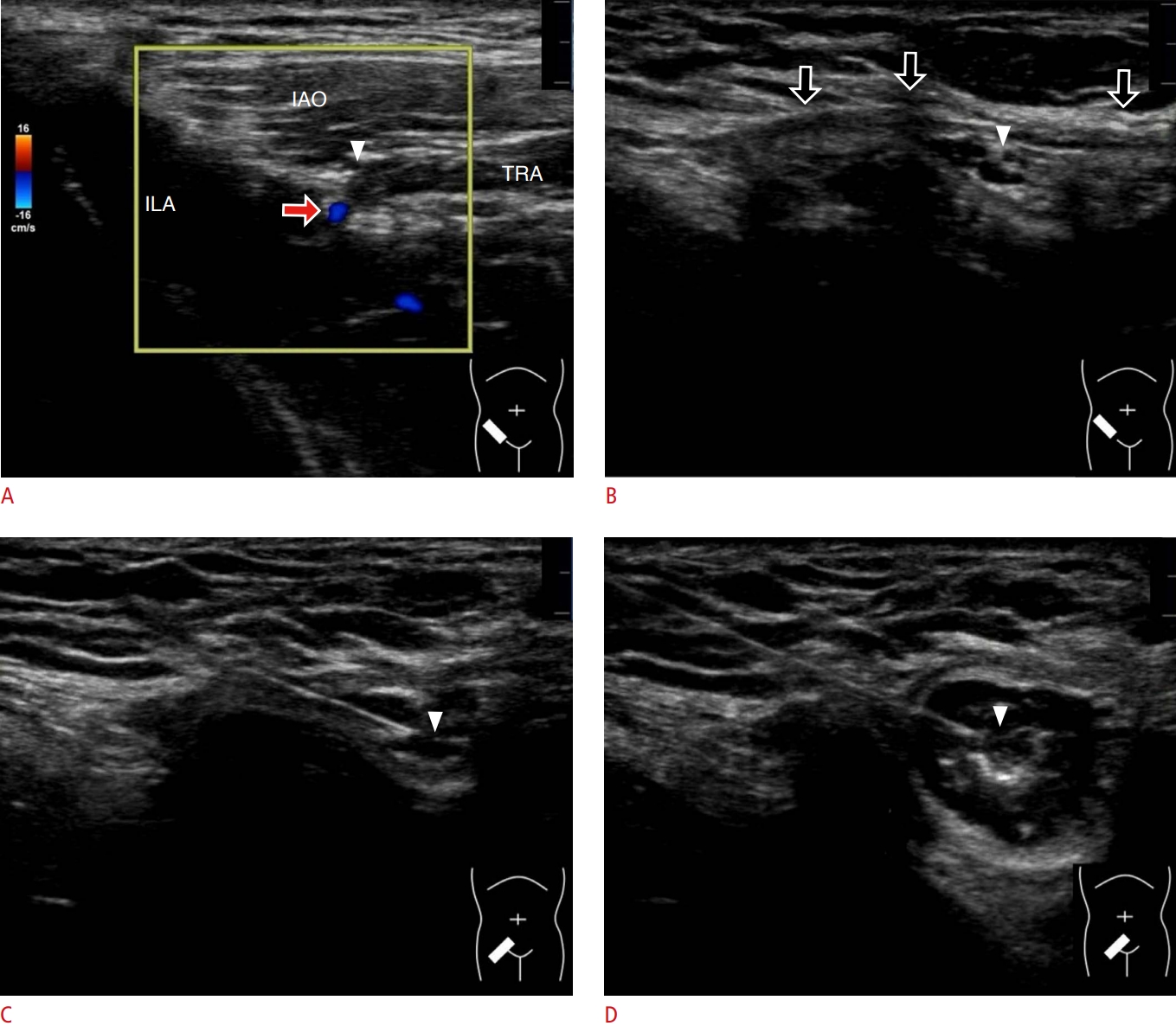
The inferior epigastric artery plays a crucial role in differentiating between indirect and direct inguinal hernias. To identify this artery, the linear transducer is placed in the horizontal plane of the lower abdomen near the midline. The artery can be recognized in its short axis under the posterior rectus sheath (Fig. 2A). Moving the transducer in a superior-medial to inferior-lateral direction reveals the location where the artery merges with the external iliac artery (Fig. 2B, Video clip 1).
The deep inguinal ring constitutes the proximal opening of the inguinal canal. It is located lateral to the junction between the inferior epigastric artery and the external iliac artery [4]. Pivoting the transducer along with the external iliac artery enables clear visualization of the cross-section of the inguinal canal (Fig. 2C). In men, the inguinal canal has a compound tubular appearance (spermatid cord) and contains the vas deferens and testicular vessels (Fig. 2D). Recognizing the inguinal canal is not easy in women, since the round ligament is the only visible structure inside the canal.
Ultrasonography of Indirect Inguinal Hernia
In patients with indirect hernia, the hernia sac protrudes through the deep inguinal ring toward the inguinal canal (Figs. 3, 4). Dilatation of the inguinal canal can also be visualized (Video clips 2, 3). In addition to the structures normally present inside the canal, the omental fat, small bowel, colon, appendix, ovary, urinary bladder, and ureter can also be observed [7]. The invaginated tissues push the spermatic cord or the round ligament against the wall of the inguinal canal. Free fluid can be observed occasionally at the caudal end of the hernia sac. Peristalsis may occur if the herniated contents include the bowels. An increase in the power Doppler activities of the herniated bowel is considered an early sign of strangulated hernia. In the late stage of strangulated hernia, vascular flow may not be detected due to ischemia [8].
During the evaluation of the hernia sac, the transducer should be moved from the deep inguinal ring to the scrotum in men and to the labia majora in women. In healthy individuals, the integrity of the inguinal canal can be preserved by contraction of the external abdominal oblique muscle, which approximates the anterior and posterior walls of the canal [5]. In patients with incomplete closure of the processus vaginalis (a reflected portion of the parietal peritoneum), increased intra-abdominal pressure forces various intra-abdominal contents to enter the inguinal canal, causing indirect hernia. Therefore, the Valsalva maneuver is helpful in reproducing the symptoms if patients are asymptomatic under static conditions (Fig. 5). However, some cases of inguinal hernia are not reproduced only by the Valsalva maneuver. Changing from a supine position to an erect position should be performed if the finding for hernia is negative during the Valsalva maneuver. This is also the advantage of US over CT for the detection of inguinal hernia [9].
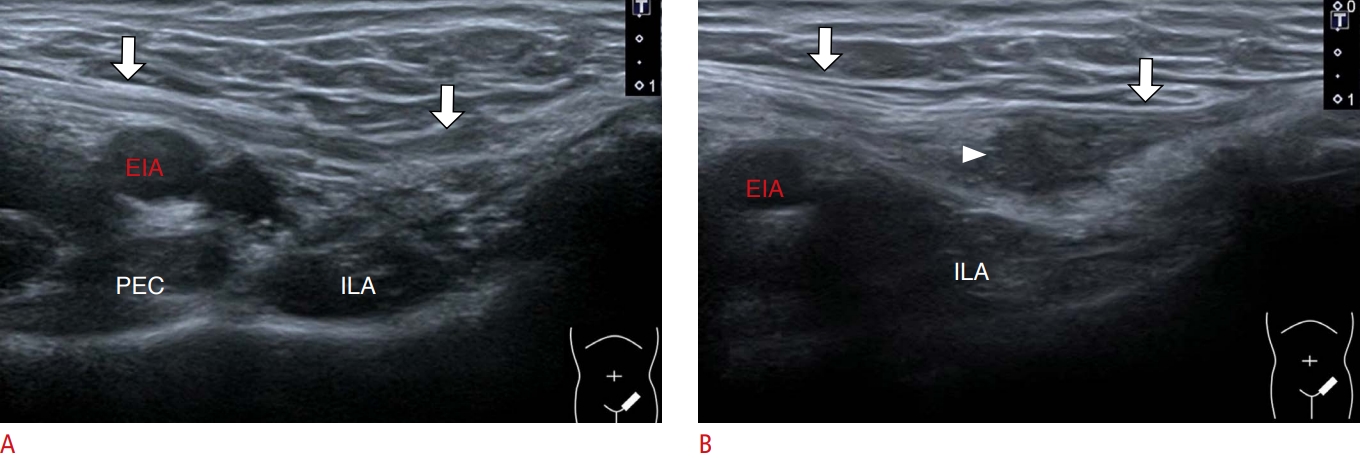
Indirect inguinal hernia is less common in women than in men. The canal of Nuck is a patent processus vaginalis in the female population [10]. Hydrocele is considered the most prevalent abnormality of this canal [10], as will be discussed in the subsequent section. Unlike the male population, there are no tubular structures such as the vas deferens and significant vascular structures such as testicular vessels in the female inguinal canal. Therefore, the use of grayscale or power Doppler US to recognize the inguinal canal is more challenging in female than male patients. The authors suggest that the investigator can place the transducer in the short-axis view to examine the inguinal ligament, which is cranial to the inguinal canal (Fig. 6, Video clip 4). If the hernia sac cannot be visualized along the course of the inguinal ligament during provocative maneuvers, indirect inguinal hernia can be excluded.
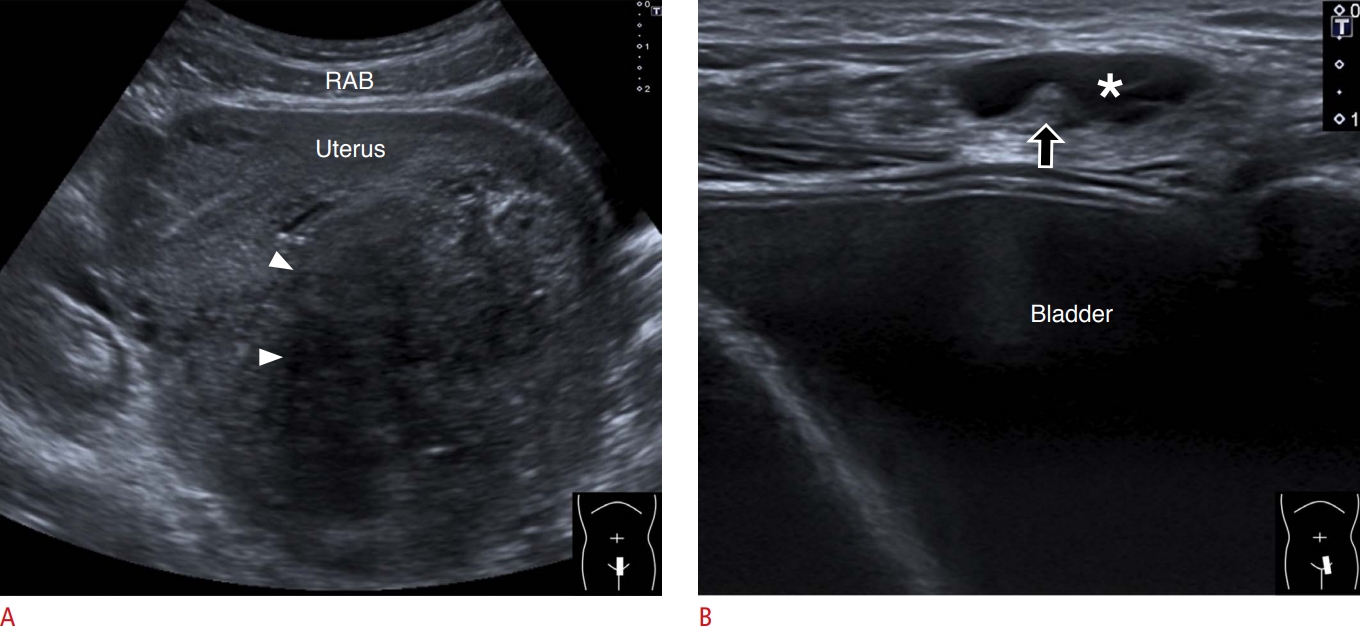
Herniation of the urinary bladder is observed in only 1%-4% of inguinal hernias and is more prevalent in men aged above 50 years [11,12]. US images may show a fluid-filled sac emerging from the inguinal region. The tract that connects the lesion and the urinary bladder can occasionally be identified (Fig. 7). If the hernia sac is large enough, a mass may be recognized over the scrotal region or the labia majora. Dynamic compression enables the visualization of changes in the size of the hernia sac. Similarly, repeated scanning after urination may reveal a reduction in the sac volume. The aforementioned tips can help physicians differentiate bladder hernias from fluid accumulation inside the processus vaginalis (Fig. 8).
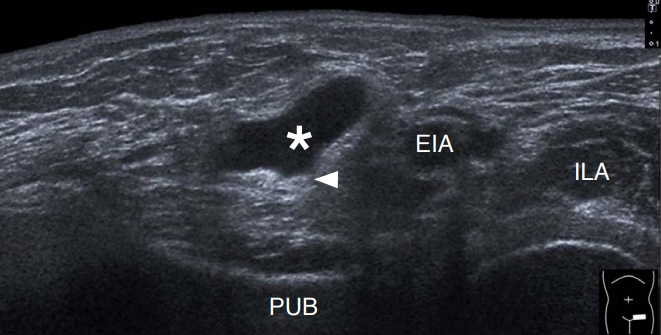
In patients with incomplete closure of the processus vaginalis, another common pathology is hydrocele, which is derived from the collection of serous fluid inside the inguinal canal. Inguinal hydrocele can be classified into communicating or non-communicating types. In communicating hydrocele, a tract that links the peritoneal cavity and the scrotum in men or the canal of Nuck in women can be recognized (Fig. 9) [10]. In non-communicating hydrocele, an anechoic fluid collection is separated from the peritoneal cavity or from the scrotum in men and from the canal of Nuck in women [10]. On US, little variation in the size of the hydrocele is observed during the Valsalva maneuver.
Ultrasonography of Direct Inguinal Hernia
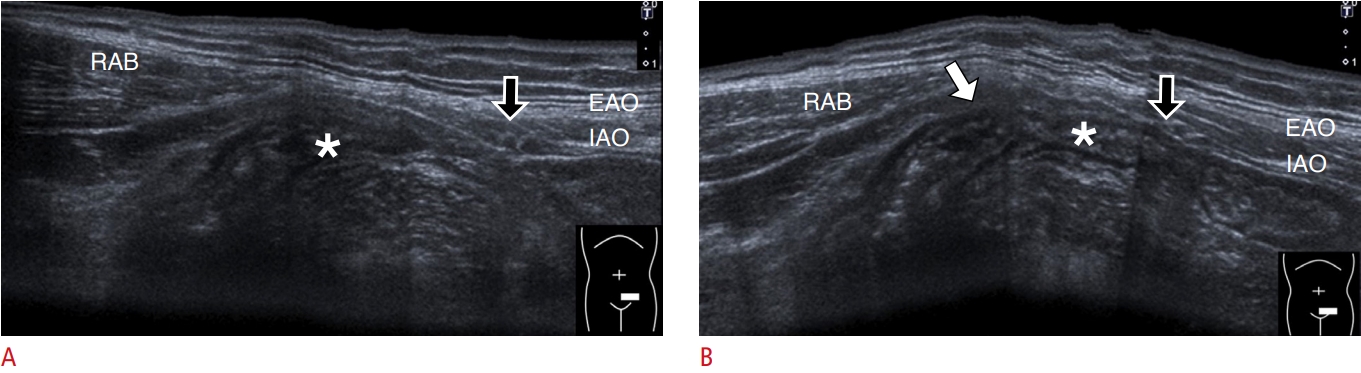
Unlike the indirect type, direct inguinal hernia is commonly seen bilaterally. The risk of strangulation is also lower in direct inguinal hernia than in indirect hernia [5]. Weakness of the abdominal wall muscles and thinning of the adjacent fasciae predispose the individuals to this type of hernia. Degeneration of the transversalis fascia plays an important role in the development of direct inguinal hernia. Therefore, its incidence increases with age [13]. During evaluation, the transducer can be placed in the horizontal plane above the inguinal ligament. Hesselbach’s triangle is a fat-filled space between the lateral edge of the rectus abdominis muscle and the inferior epigastric artery [4]. The sonographer should scrutinize the entire Hesselbach’s triangle for a fat-containing or bowel-containing hernial sac (Video clip 5). As the hernial sac is likely to be less prominent in the supine position, a standing posture with a simultaneous Valsalva maneuver might be helpful for detecting the hernia more easily (Fig. 10).
Ultrasonography in Postoperative Follow-up and Pain Management
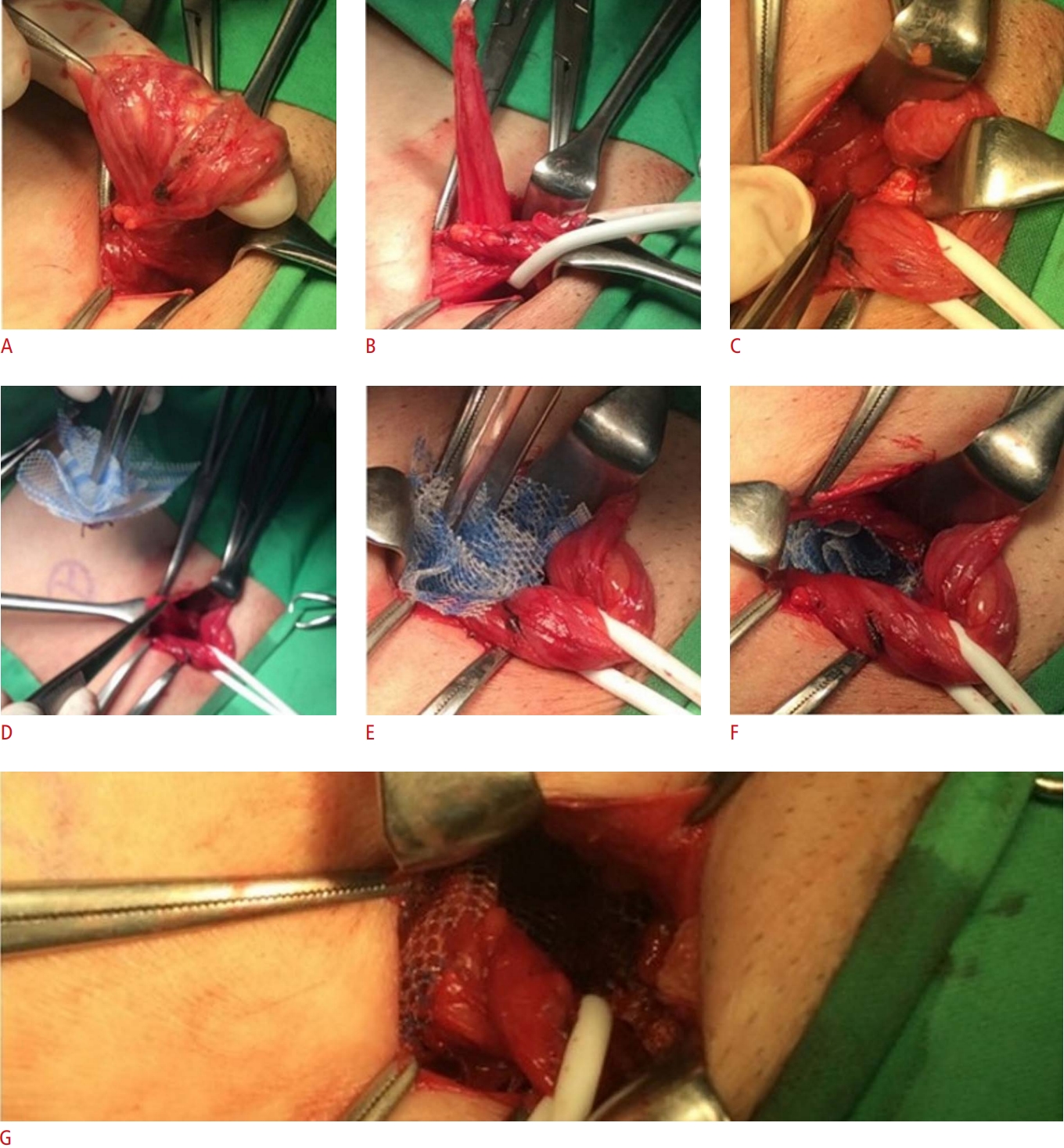
Not all patients with hernia require or undergo surgery. The indications for an emergent operation mainly include incarceration and strangulation of the hernia sac. In the past, traditional tissue repair has been widely used, which involves reduction of the protruded contents back to the abdomen, excision of the hernia sac, and closure of the defect. However, due to high recurrence, tension-free methods have emerged as the mainstream techniques. The mesh plug method (inserting a cone-shaped mesh to plug the opening of the hernia defect and placing a synthetic mesh to reinforce the posterior wall of the inguinal canal) has been adopted at the authors’ institution (Fig. 11). A recent meta-analysis [15] revealed that open mesh repair led to a significantly lower incidence of recurrence than suture repair.
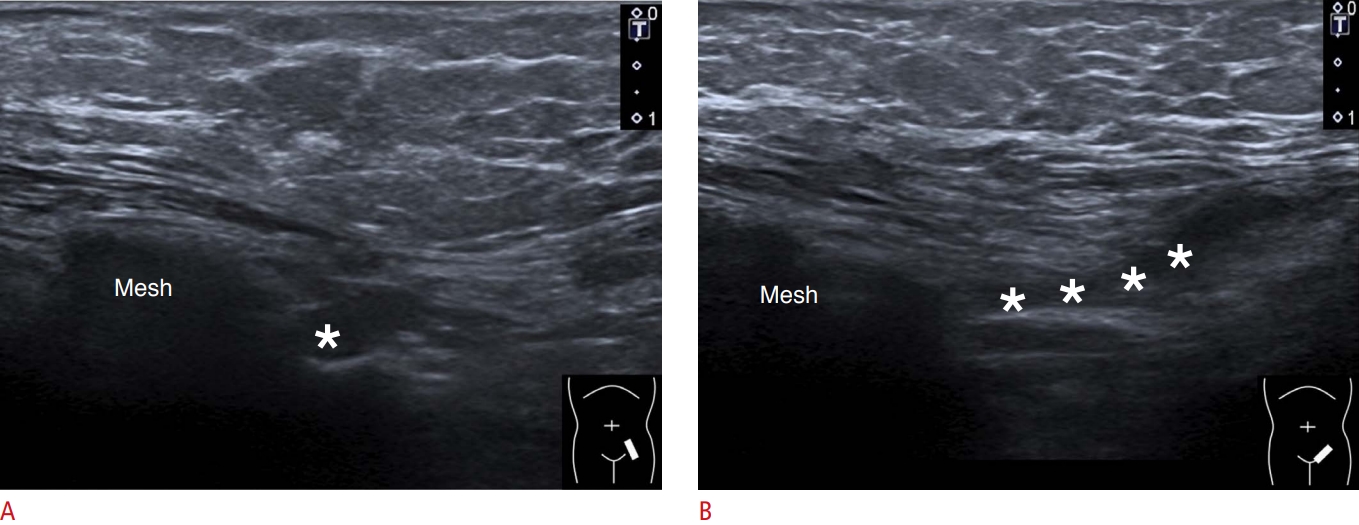
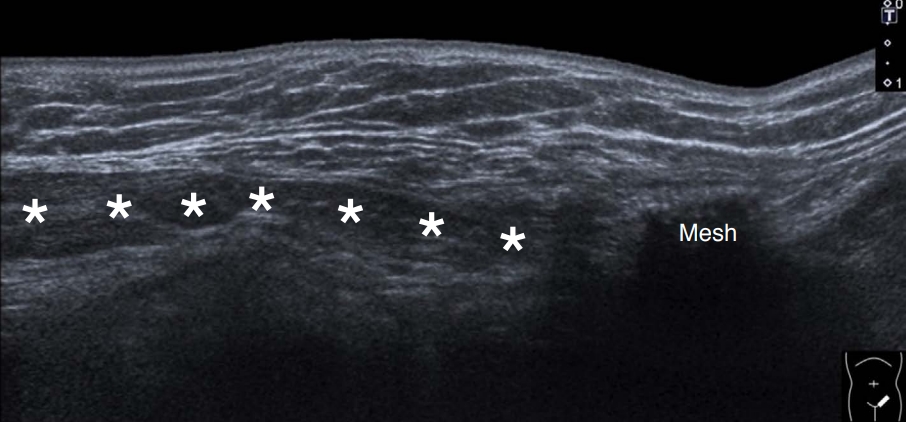
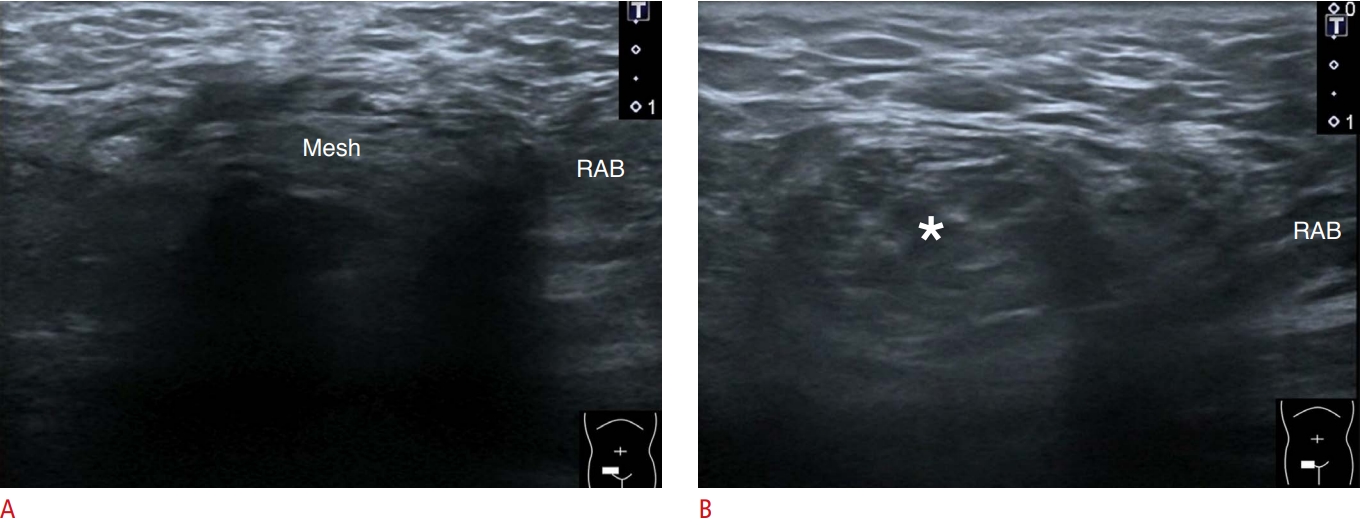
Seroma and hematoma are two common complications after hernia surgery [16]. Seroma appears as an anechoic fluid collection on US imaging and is likely to resolve approximately 1 month after surgery. Postoperative hematoma may exhibit mixed echogenicity with comparable fluid accumulation (Fig. 12). US is also helpful in the evaluation of postoperative recurrence of hernia. The synaptic mesh casts an acoustic shadow deep into it on US imaging. Displacement or disintegration of the mesh is a common cause of hernia recurrence. The hernia sac can emerge from the edge of the mesh. In cases of recurrence of indirect hernia, the enlarged inguinal canal can sometimes be visualized from the inferior lateral border of the mesh to the pubic symphysis (Figs. 13, 14). In patients with recurrence of direct inguinal hernia, the hernia sac is usually present at the inferior border of the mesh due to gravity (Fig. 15).
Some patients may develop postoperative pain lasting for more than 3 months after surgery [17]. Its pathogenesis is multifactorial, comprising perioperative damage to the regional nerve(s) and persistent local inflammation. Another possibility is the entrapment of the regional nerves by the implanted mesh. US-guided nerve block and radiofrequency ablation can be used before other invasive approaches [18], targeting the ilioinguinal nerve (Fig. 16, Video clip 6) and the genital branch of the genitofemoral nerve. The iliolingual nerve can be identified at the fascial plane between the transverse abdominis and internal abdominal oblique muscles by placing the transducer over the anterior superior iliac spine and pointing its medial edge toward the umbilicus [19]. The genital branch of the genitofemoral nerve is located inside the inguinal canal and can be blocked by distributing the injectate around the spermatic cord or the round ligament. Mesh removal and neurectomy are considered the ultimate options for patients with recalcitrant pain.
Differential Diagnosis
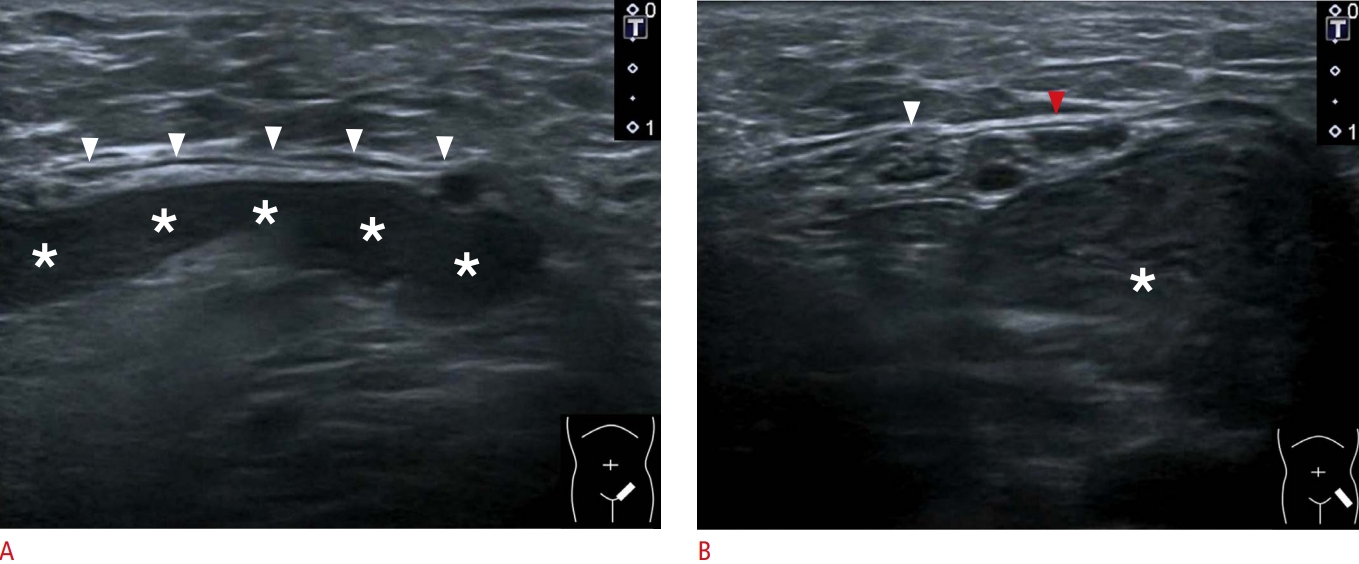
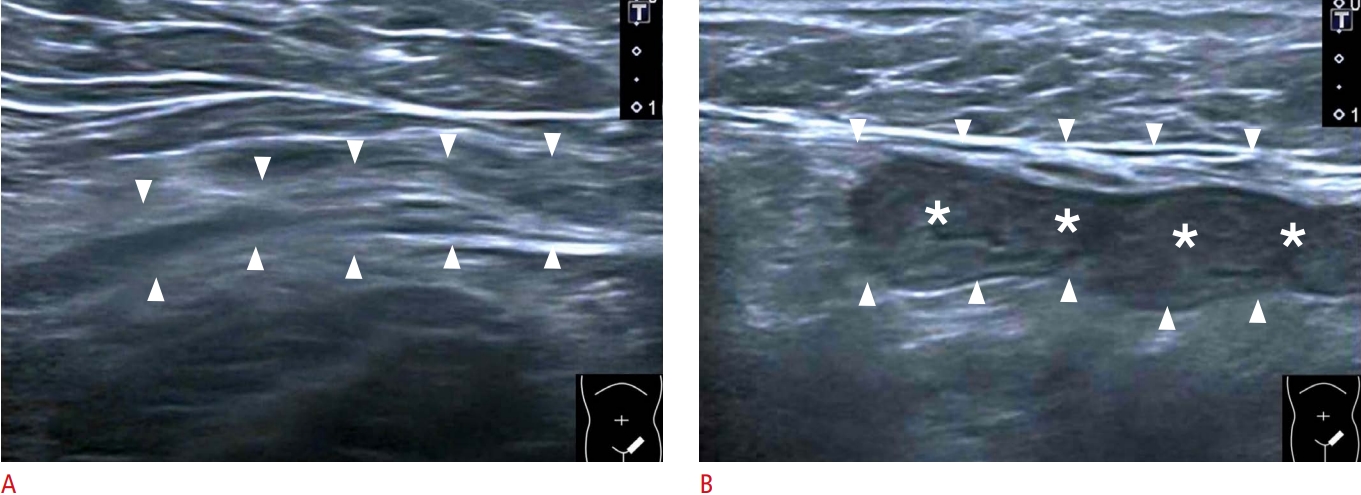
Regarding the differential diagnosis, hydrocele should be the top differential diagnosis of inguinal hernia, especially in neonates or infants. Hydrocele is discussed in the previous section ("Ultrasonography of Indirect Inguinal Hernia"), and the discussion is not repeated here. In adult patients, lymphadenopathy (Fig. 17A) and tumors such as lipomas (Fig. 17B) are common differential diagnoses for palpable inguinal masses. Endometriosis (presence of endometrial tissue outside the uterus) can manifest as a palpable mass in the inguinal region [20] but is rare. Extra-pelvic endometrial tissues can be found in the cutaneous, subcutaneous, and intramuscular layers. If they involve the inguinal canal and the round ligament, symptoms such as indirect inguinal hernia may ensue. Since the ectopic tissues are firmly attached to the canal wall, they do not migrate during a change in position or during the Valsalva maneuver. Unlike typical indirect inguinal hernias, which are mostly asymptomatic, endometriosis is usually painful and its severity varies according to the menstrual cycle.
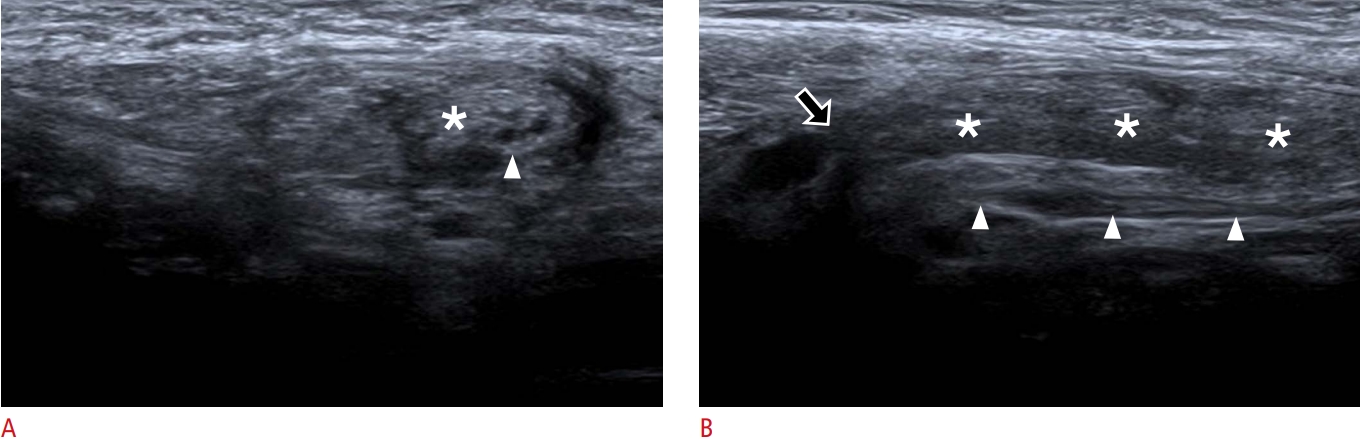
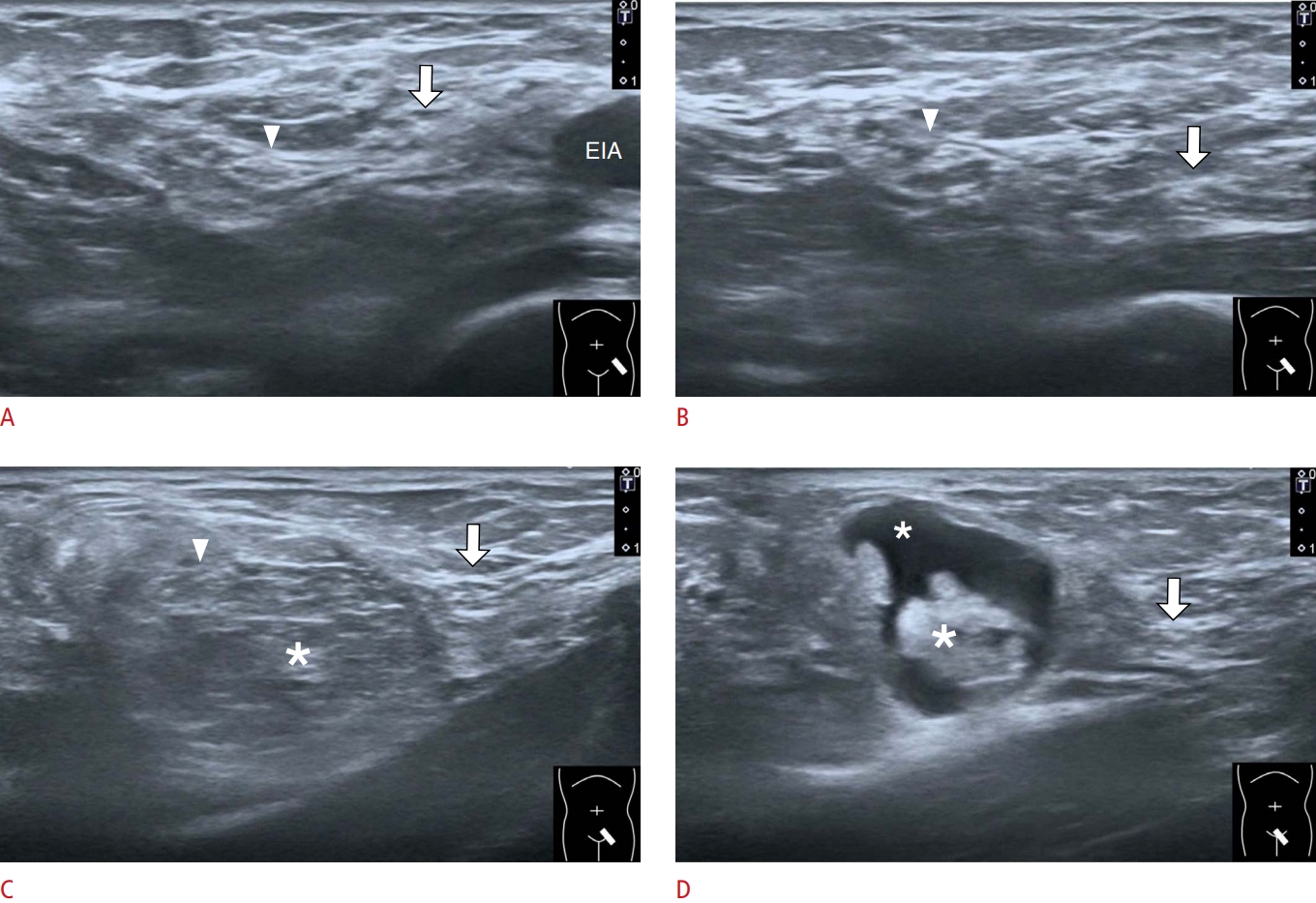
On US, inguinal endometriosis appears as a hypoechoic nodular mass inside the inguinal canal or next to the inguinal ligament (Fig. 18). A petechial increase in power Doppler activity is commonly observed inside the lesion (Fig. 19). Dynamic mobilization of the transducer reveals firm attachment of the mass to the adjacent tissues. The thickness of the endometrial tissues may vary in different phases of the menstrual cycle.
Massive ascites may be seen as bilateral swelling of the inguinal area and sometimes accompany cord or scrotal hydrocele. The causes of ascites are multifaceted, including malignancy, malnutrition, cirrhosis, chronic heart failure, and chronic renal failure. Ascites can be transudative (protein content <25 g/L) or exudative (protein content >25 g/L) [21]. Transudate usually appears as an anechoic homogenous fluid collection with posterior enhancement on US imaging (Fig. 20). In contrast, exudate contains various amounts of debris and internal septa. US-guided aspiration of ascites is helpful for determining its biochemical profile, as well as for symptomatic relief.
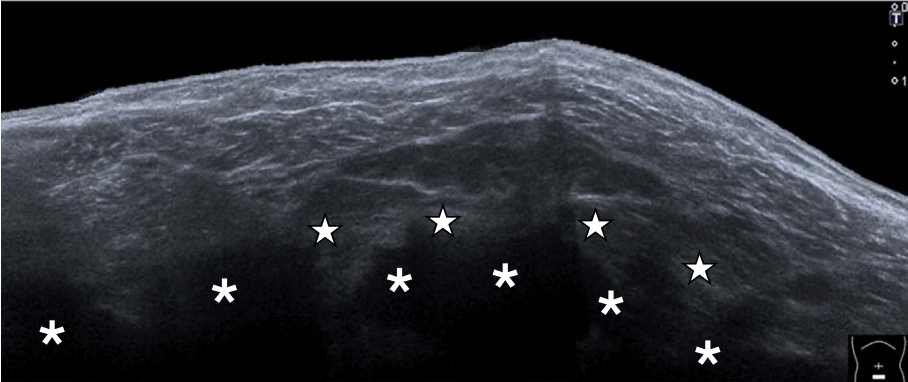
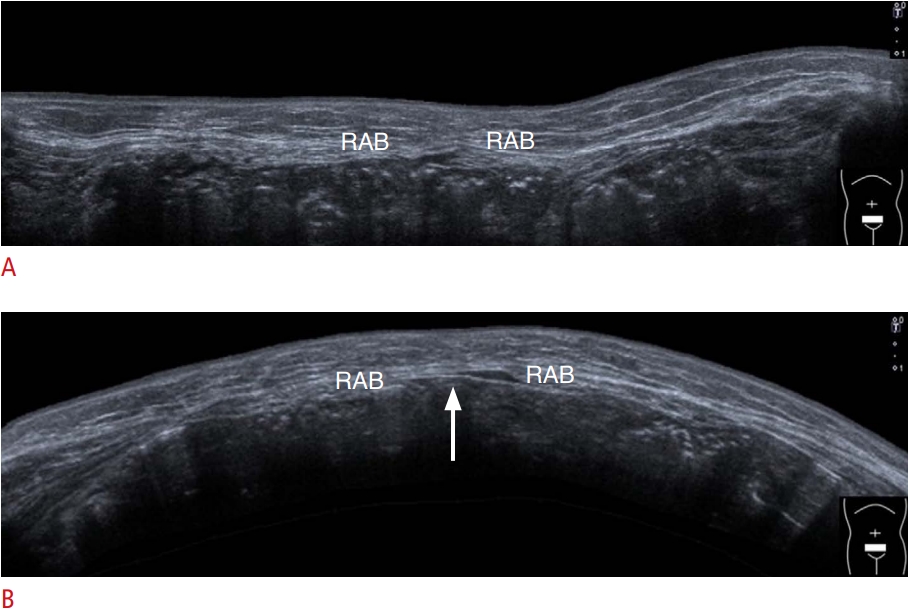
Sarcopenia (decreased muscle mass and function) is prevalent in the aging population [22,23]. In a previous study, thinning of the rectus abdominis, external oblique, and internal oblique muscles was observed on US imaging in 103 middle-aged and older healthy women [24]. Weakness of the abdominal wall muscles can be observed after abdominal surgery. In case of severe involvement, the lower abdominal region protrudes during standing, mimicking bilateral inguinal hernia (Fig. 21).
Conclusion
The present review demonstrates the usefulness of US imaging in the evaluation of inguinal hernia. The inferior epigastric artery is the most important landmark for differentiating between indirect and direct inguinal hernias. Dynamic US imaging combined with postural changes and the Valsalva maneuver is helpful for symptom reproduction. In patients undergoing hernia repair surgery, US imaging is helpful for detecting postoperative complications and recurrence of hernia.




 Download Citation
Download Citation PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Full text via PMC
Full text via PMC



