

 Print
Print facebook
facebook twitter
twitter Linkedin
Linkedin google+
google+

Introduction
Radiofrequency ablation (RFA) has been used to manage metastatic colorectal cancer (CRC) in the liver of patients ineligible for hepatic resection. However, one of the drawbacks of RFA is frequent local tumor progression (LTP) compared to hepatic resection. Tumor size, ablative margin, and perivascular or subcapsular tumor location have been associated with LTP after RFA [1-3].
Meanwhile, tumors up to 3 cm in diameter are generally considered good candidates for RFA of colorectal liver metastases (CLM) [4,5]. As RFA has evolved in the last decade, RFA with multiple or perfusion electrodes is currently being used to create a sufficient ablative margin. Recently, no-touch RFA, wherein multiple radiofrequency electrodes are placed outside the tumor, has become popular. As no-touch RFA can create a larger ablation zone than conventional tumor-puncturing RFA [6], it is easy to create ablative margins larger than 1.0 cm all around the index tumor, which are ideal for CLM [3,7,8]. This could ensure excellent local tumor control.
Furthermore, it is expected that even perivascular tumors, which are prone to the so-called "heat-sink effect," may be overcome by these advanced RFA techniques as multiple electrodes can be placed outside the tumor near the peritumoral vessels. In addition, more accurate guidance methods, such as fusion imaging of real-time ultrasonography (US) and pre-acquired computed tomography (CT), magnetic resonance imaging (MRI), or contrast-enhanced US, are now available [9-11]. For these reasons, therapeutic outcomes after RFA using advanced techniques need to be re-assessed using the latest clinical data. However, to the authorsŌĆÖ knowledge, no studies of RFA for CLM have reflected these recent changes.
Therefore, this study aimed to evaluate LTP-free survival (LTPFS) and overall survival (OS) after percutaneous RFA for solitary CLM <3 cm at a tertiary cancer center. The risk factors associated with poor LTPFS and OS after percutaneous RFA were also assessed.
Materials and Methods
Compliance with Ethical Standards
The Institutional Review Board of Samsung Medical Center (2021-11-100) of the authorsŌĆÖ medical center approved this retrospective study, and the requirement for written informed consent from patients was waived.
Patients
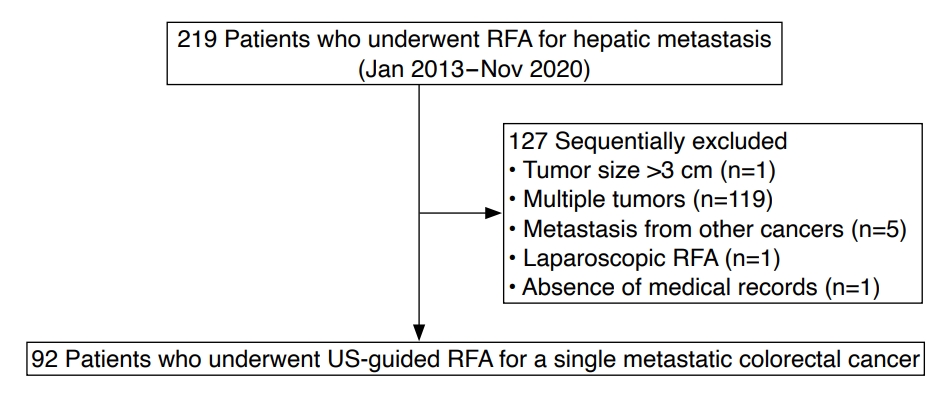
In total, 219 patients who underwent RFA for hepatic metastasis between January 2013 and November 2020 were screened retrospectively. Among them, 127 patients were excluded for the following reasons: (1) multiple metastases (n=119), (2) metastasis from cancers other than CRC (n=5), (3) tumor size >3 cm (n=1), (4) patients who underwent laparoscopic RFA (n=1), and (5) absence of electronic medical records (n=1). Finally, 92 patients who underwent US-guided RFA for a single CLM <3 cm were included. Hepatic metastasis was diagnosed based on percutaneous biopsy (n=2) or typical imaging findings of CT or MRI (n=90) (Fig. 1).
Percutaneous RFA
All RFA procedures were performed percutaneously by five radiologists who had at least 3 years of experience with RFA. The RFA procedures were performed under conscious sedation or monitored anesthesia, which was conducted under the care of anesthesiologists. Fusion imaging (volume navigation; LOGIQ E9, GE Healthcare, Chicago, IL, USA) of real-time US and CT/MRI scans were used to guide and monitor the RFA procedures [12]. Various RFA systems (VIVA RFA System, STARmed, Goyang, Korea; Jet-tip RFA System, RF Medical, Seoul, Korea) were used according to the operatorŌĆÖs preference. The aim was to achieve at least a 0.5- to 1.0-cm ablative margin around the index tumor, except in perivascular and subcapsular tumor locations.
The type and number of radiofrequency electrodes were chosen based on the tumor size and shape. In the earlier period of this study, conventional tumor-puncturing RFA was performed using a single electrode, especially for small tumors <2 cm. When using multiple electrodes (Octopus electrode, STARmed; Twins electrodes, RF Medical), centripetal RFA was performed after placing electrodes at the peripheral portion of the tumor. Gradually, no-touch RFA also started to be used as it can provide a sufficient ablative margin, leading to effective local tumor control [13]. Initially, no-touch RFA was feasible using a monopolar mode of energy delivery. The bipolar mode became available for Twins electrodes in 2018 and Octopus electrodes in 2019, respectively, and after those time points, monopolar, bipolar, or combined monopolar and bipolar modes were used. Overlapping ablation was performed when required to achieve a sufficient ablative margin. RFA procedures were continued until the echogenic zone created by RFA in the US was large enough to cover the entire tumor. The electrode path was cauterized during electrode removal at the end of the RFA procedure.
Assessment of Treatment Response and Complication
The treatment response and complications were evaluated using contrast-enhanced CT within 12 hours after the procedure. The treatment was considered a technical success if the RFA zone entirely covered the index tumor on CT [14]. A second RFA session was attempted within 24 hours after the first RFA session when a residual unablated tumor was noted on CT images. Technical efficacy was assessed through 1-month follow-up CT or MRI.
A major complication was defined as an event that led to substantial morbidity and disability that increased the level of care, resulting in hospital admission or a substantially lengthened hospital stay. All other complications were considered minor [14].
Follow-up
Follow-up contrast-enhanced CT/MRI was performed 1 month after the initial treatment and every 3 to 6 months thereafter. Chest CT, serum carcinoembryonic antigen, carbohydrate antigen 19-9, and liver function tests were also performed. LTP was defined as the appearance of tumor foci at the edge of the ablation zone [14].
Assessment of Therapeutic Outcomes
The size of the ablation zone was measured on immediate post-RFA CT. The maximum (Dmax) and minimum (Dmin) diameters of the ablation zone were measured from axial CT images of the portal phase and the longest vertical diameter (Dv) from sagittal or coronal images. The ablation volume was calculated by the formula for ellipsoid lesion (ablation volume=ŽĆ(Dmax├ŚDmin├ŚDv)/6) [17].
Therapeutic outcomes, including LTPFS and OS, were assessed. LTPFS was defined as the time interval between the initial RFA and the first radiographic evidence of LTP [5,18]. OS was defined as the time from the initial treatment to death or the last date of a follow-up visit before November 22, 2020.
Statistical Analyses
Patient demographics and clinical characteristics were analyzed using descriptive statistics. They were presented as numbers with percentages for categorical variables and medians with ranges or means with standard deviations for continuous variables. The ratios of the longest diameter of the ablation zone and tumor size and those of the ablation volume and tumor volume were compared between the no-touch RFA and tumor-puncturing RFA groups using the Wilcoxon rank-sum test. Survival curves were generated using the Kaplan-Meier method, and differences between curves were compared using the log-rank test.
Univariable and multivariable analyses were performed to identify risk factors for LTPFS or OS using Cox proportional-hazard regression models. The risk factors for LTPFS were assessed using the variables with patient-, tumor-, and RFA-related factors. The interaction effect between the T stage and the method of electrode placement was assessed through a post-hoc analysis to evaluate the interaction effect of the two variables on LTPFS. Variables with P<0.1 in the univariable analysis and a combination of the two variables related to the interaction effect were included in the multivariable analysis.
The risk factors for OS were also assessed using a Cox regression analysis with the same variables as for LTPFS. The interaction effect between the T stage and the method of electrode placement was also assessed with post-hoc analysis to evaluate the interaction effect of the two variables on OS. Statistical analyses were performed using R version 3.5.0 (The R Foundation for Statistical Computing, Vienna, Austria). Statistical significance was set at P<0.05.
Results
Baseline Characteristics
The baseline characteristics of the patients are summarized in Table 1. Of the 92 patients included, 68.5% were men. The mean patient age was 60.2 years. The T and N stages of primary CRC were as follows: T1-T3 (70.7%), T4 (27.2%), N0 (31.5%), and N1-N2 (65.2%), respectively. After primary tumor control of CRC, the disease-free interval was Ōēż12 months in 76.1% of patients. The number of radiofrequency electrodes used for RFA was as follows: 1 (32.6%, 30/92), 2 (44.6%, 41/92), and 3 (22.8%, 21/92). The number of overlapping ablations was as follows: 1 (19.6%, 18/92), 2 (21.7%, 20/92), and 3 or more (58.7%, 54/92). In terms of electrode placement, no-touch RFA was performed in 22.8% of patients, and tumor-puncturing RFA was performed in 77.2%.
Treatment Response and Complications
Technical success was achieved in 91 of 92 patients (98.9%). A residual unablated tumor was found in one patient on immediate post-RFA CT images, and a second RFA session was performed, which led to successful local tumor control. Technical efficacy was achieved in all 92 patients (100%) in the 1-month follow-up CT images.
Major complications were found in three patients after RFA. These included biliary sepsis (n=1), subcapsular hematoma (n=1), and large biloma (n=1). All three patients recovered fully after conservative treatment. Minor complications were found in four patients: biloma (n=1), subsegmental infarction (n=2), and diaphragmatic thermal injury (n=1).
Ablation Zone
The median longest diameter of the ablation zone was 4.6 cm (range, 3.1 to 6.3 cm) in the no-touch RFA group and 3.9 cm (range, 1.9 to 7.3 cm) in the tumor-puncturing RFA group. The median volume of the ablation zone was 24.5 cm3 (range, 9.5 to 58.1 cm3) in the no-touch RFA group and 16.3 cm3 (range, 2.7 to 131.7 cm3) in the tumor-puncturing RFA group (P=0.016). The ratio of the longest diameter and the volume between the ablation zone and those of the tumors between the no-touch RFA and tumor-puncturing RFA groups are summarized in Table 2. The ratio of the longest diameter was significantly larger in the no-touch RFA group than the tumor-puncturing RFA group (P=0.035). The volume ratio had a tendency to be larger in the no-touch RFA group than in the tumor-puncturing RFA group, but it did not reach statistical significance (P=0.114).
Local Tumor Progression-Free Survival
The median follow-up period was 20.0 months (range, 1.8 to 90.3 months). During follow-up, LTP was observed in 12 of 92 patients (13.0%). The cumulative LTPFS rates at 1, 3, and 5 years were 92.4%, 83.4%, and 76.5%, respectively.
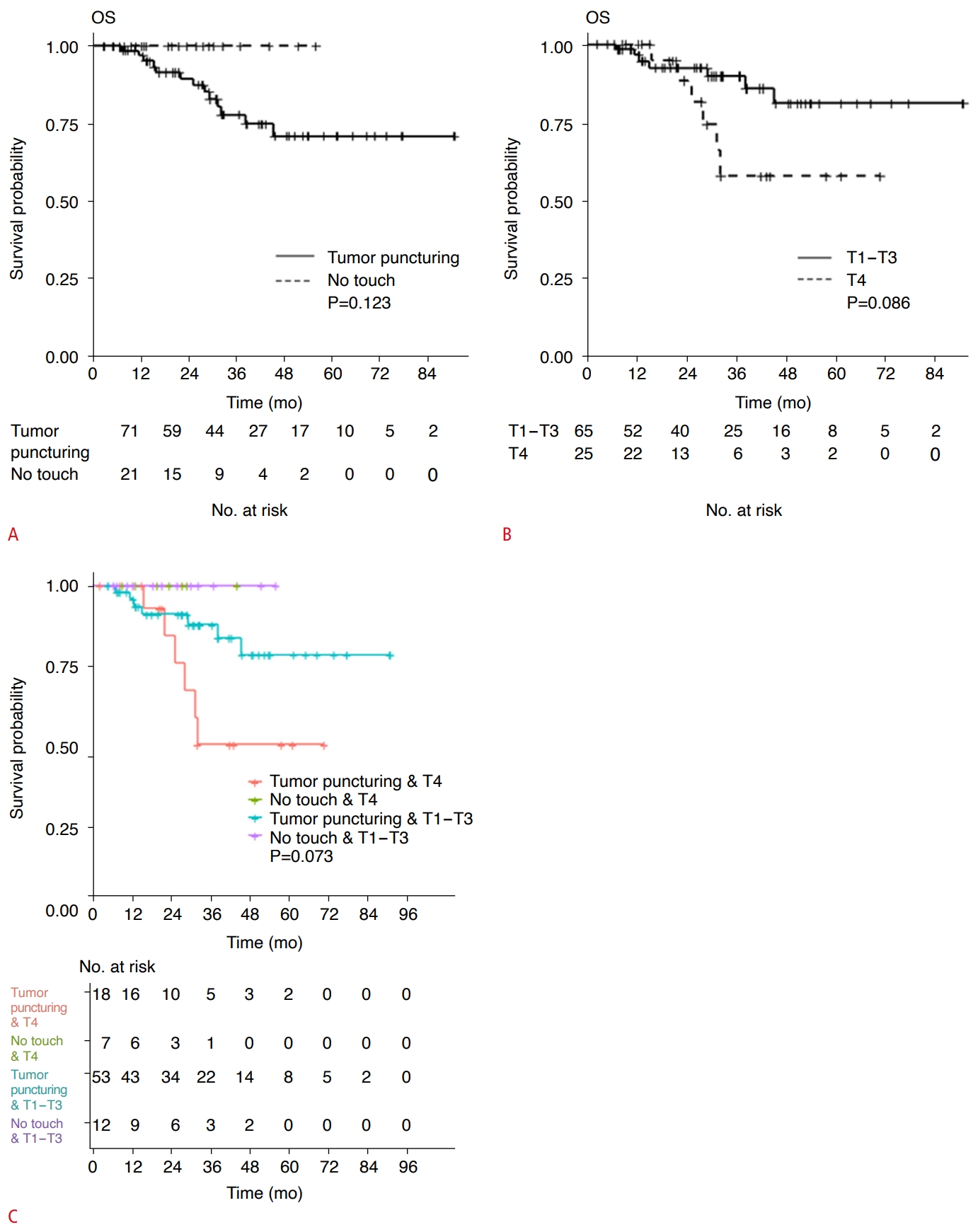
The univariable Cox proportional hazard regression model revealed that the T stage of the primary tumor was a risk factor for LTPFS (P=0.048). The method of electrode placement (P=0.071) and patient age (P=0.066) showed borderline significance as risk factors for LTPFS (Table 3, Figs. 2, 3). As LTPFS tended to be higher with no-touch RFA than with tumor-puncturing RFA, the possibility of an interaction effect between the method of electrode placement and the T stage of the primary tumor was evaluated, and an interaction effect was found between the two variables. The combined group of tumor-puncturing RFA and a T4 stage tumor was associated with poor LTPFS (hazard ratio, 10.3; 95% confidence interval [CI], 1.2 to 1,345.5; P=0.029), compared to the reference group, no-touch RFA and T1-T3 stage (Table 4, Fig. 4). Multivariable Cox regression analyses showed that the combination of tumor-puncturing RFA and a T4 stage tumor was associated with poor LTPFS (hazard ratio, 3.3; 95% CI, 1.1 to 10.2; P=0.037) (Table 3).
Discussion
This study analyzed the treatment outcomes of percutaneous RFA of a single CLM <3 cm in size. The results showed an interaction effect of the method of electrode placement and the T stage of primary CRC on LTPFS. The group with both tumor-puncturing RFA and a T4 stage tumor had poorer LTPFS than those with no-touch RFA and T1-T3 stages. The multivariable analysis also showed that the combination of tumor-puncturing RFA and a T4 stage tumor was an independent risk factor for poor LTPFS. However, no interaction effect of the variables mentioned above was found on OS, and there were no significant risk factors associated with poor OS.
A sufficient ablative margin has been reported to be critical for preventing LTP after RFA [1,8,19,20]. When ablative margins were >10 mm, no LTP was found after the RFA of CLM [3,5]. During the study period between January 2013 and November 2020, we became aware of this fact and gradually adopted centripetal RFA or no-touch RFA using multiple electrodes to create a sufficient ablative margin. For this reason, multiple electrodes were used in 80.4% (74/92) of patients in this study, and no-touch RFA was performed in 22.8% (21/92). Of note, LTP was not found in patients who underwent no-touch RFA, which may be attributed to the larger size of the ablation zone with no-touch RFA than that of tumor-puncturing RFA [6]. Consequently, the cumulative LTPFS rates at 1, 3, and 5 years were 92.4%, 83.4%, and 76.5%, respectively. These results appear comparable or superior to the previously reported outcomes of RFA for CLM [2,3,5].
During no-touch RFA, multiple electrodes are inserted outside the tumor boundary, and centripetal ablation of the tumor is feasible. This type of energy deposition can help obtain a sufficient ablation margin and obliterate feeding and draining vessels in the earlier period of the RFA process. Furthermore, as the electrodes are not in direct contact with the tumor, they may prevent tumor spread around the tumor, and there is no risk of tract seeding. In a recent multicenter prospective study [13], no-touch RFA led to excellent local tumor control after RFA of hepatocellular carcinomas <2.5 cm in size, and the cumulative LTP rate at 2 years was only 1.6%. CLM may also benefit from no-touch RFA, as confirmed in this study.
An interaction effect was found between electrode placement and the T stage of primary CRC on LTPFS. The group with both tumor-puncturing RFA and a T4 stage tumor showed poor LTPFS (hazard ratio, 10.3; 95% CI, 1.2 to 1,345.5; P=0.029) compared to the reference group of no-touch RFA and T1-T3 stages of primary CRC. In addition, in patients undergoing RFA for CLM, the combination of tumor-puncturing RFA and a T4 stage tumor was an independent risk factor for poor LTPFS. Although the association between the T stage of primary CRC and local tumor control of RFA for CLM is not clearly understood, an advanced T stage of primary CRC is known to be associated with poorly differentiated tumors [21]. It has been postulated that an advanced T stage of primary CRC may be associated with aggressive tumor biology of CLM due to poor differentiation, which may yield poor LTPFS after RFA for CLM. Similarly, poorly differentiated hepatocellular carcinoma was identified as a risk factor for LTP after percutaneous RFA [22]. Interestingly, no LTP was found in our study even in patients with T4 stage tumors when no-touch RFA was performed (Fig. 4).
Tumor size and a perivascular or subcapsular location of the CLM are well-known factors affecting local tumor control [1-3,5,23]. Han et al. [2] reported that a tumor size of Ōēź2 cm was associated with LTP after RFA. In addition, perivascular tumors are known to have a relatively increased risk of ablation failure and LTP due to the "heat-sink" effect [24]. Subcapsular tumors are also associated with higher LTP and shorter LTPFS [23,25]. However, tumor size and perivascular or subcapsular location of the tumors were not significantly associated with LTP after RFA in the present study. It is postulated that a sufficient ablative margin obtained by using centripetal RFA or no-touch RFA with multiple electrodes in some cases may have resulted in favorable local tumor control in our study.
It is known that large tumor size (>3 cm) and more than one site of extrahepatic disease are poor prognostic factors for OS [5]. However, no factors were found to be significantly associated with OS in this study. Given that tumors smaller than 3 cm were included in the present study, RFA for CLM <3 cm seemed to lead to good survival outcomes when an aggressive ablation strategy was adopted. In addition, as only three of the 92 patients had extrahepatic disease, it may have been difficult to ascertain statistical significance. Further studies with a larger study population are warranted to verify these results.
The present study had several limitations. First, it was a retrospective study performed at a single medical center. Therefore, selection bias may have occurred. Second, although the ablative margin is known to be a factor associated with LTP, it was not assessed because there is no standardized method for evaluating the ablative margin, and an accurate assessment of the ablative margin is sometimes challenging when the index tumor is not demarcated within the ablation zone. However, the effect of a sufficient ablative margin could be indirectly inferred from the difference in ablation zone size between no-touch RFA and tumor-puncturing RFA. This assumption is supported by a randomized controlled trial between no-touch RFA and conventional tumor-puncturing RFA, in which no-touch RFA provided a larger ablative margin than conventional tumor-puncturing RFA [6]. Third, this study only included patients with a single hepatic metastasis, as we intended to evaluate whether LTPFS and OS after RFA are affected by the specific tumor location through a tumor-based analysis. Fourth, the diagnosis of hepatic metastasis was made based on imaging findings, not a histologic diagnosis, in almost all cases. Although this policy reflects actual clinical practice, patients with a false-positive diagnosis of metastasis may have been included in this cohort.
In conclusion, both LTPFS and OS were promising after percutaneous RFA of a single CLM. LTP was not observed in patients who underwent no-touch RFA. The group with both tumor-puncturing RFA and a T4 stage tumor showed poor LTPFS. No risk factors were identified for poor OS.


 Download Citation
Download Citation PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Full text via PMC
Full text via PMC



