

 Print
Print facebook
facebook twitter
twitter Linkedin
Linkedin google+
google+

Introduction
H├╝rthle cells are large polygonal cells with eosinophilic granular cytoplasm due to dense mitochondrial content, which may also be described as oncocytic or oxyphilic cells [1,2]. They present with a wide range of pathologic entities, including Hashimoto thyroiditis, chronic lymphocytic thyroiditis, adenomatous goiter with H├╝rthle cell metaplasia, and H├╝rthle cell neoplasms (HCNs) [3].
The term "HCN" has been used to describe encapsulated tumors that contain a minimum of 75% H├╝rthle cells. HCNs are classified as benign H├╝rthle cell adenomas (HCAs), malignant H├╝rthle cell carcinomas (HCCs), and HCNs of uncertain malignant behavior (UMB) [2,4-7]. HCAs do not show capsular or vascular invasion, while HCCs demonstrate entire-thickness capsular invasion and/or the presence of vascular invasion by tumor cells. HCNs of UMB are characterized by an equivocal degree of capsular invasion with absent vascular invasion [5].
The clinical behavior of HCNs has been a topic of substantial debate. HCCs have been considered to behave in a more aggressive fashion than other well-differentiated thyroid cancers [8,9]. While these cancers are traditionally grouped with follicular thyroid cancers, they appear to differ clinically, with a higher rate of nodal metastases, a decreased avidity for I-131, and a lower survival rate [9-11]. They present unique genetic, pathologic, and clinical features different from those of follicular neoplasms [11]. Due to the clinical uncertainty associated with these lesions, many surgeons treat them more aggressively than follicular neoplasms [12].
Several prior studies have described the sonographic appearance of HCNs. These reports have documented the typical features of HCNs as solid hypoechoic masses with a characteristic halo sign [13-17]. Fewer investigators have tried to differentiate HCCs from HCAs. There have also been some differences in the methods of collecting study populations. First, Santana et al. analyzed the characteristics of malignancy in pathologically proven HCN cases after lobectomy or thyroidectomy, and concluded that there was no significant distinguishing factor between benignity and malignancy [16]. In contrast, Lee et al. [13] and Kim et al. [18] performed pathologic and radiologic evaluation of pathologically confirmed HCN cases among lesions suspected to be HCNs on fine-needle aspiration (FNA), and reported that tumor size was a single independent predictive factor. FNA alone cannot diagnose HCN, and in this process, H├╝rthle cell-related conditions other than HCN, such as goiter with H├╝rthle cell metaplasia or Hashimoto thyroiditis, can be included [13,18]. Thus, there is a possibility that previous analyses may have contained irrelevant data, such as incidentally found HCNs. Therefore, the population of the present study was selected from pathologically proven HCN cases that could be correlated with preoperative ultrasound (US) findings. Furthermore, due to the diseaseŌĆÖs rarity, previous studies have included only small case numbers or a mixed population of patients with other etiologies of malignancy, which may have limited the applicability of their statistical analyses [13-16,19]. The primary objective of this study was to evaluate the US features that suggest malignancy in HCNs. To the authorsŌĆÖ knowledge, this is the largest study to date that has investigated various US features based on surgically proven cases.
Materias and Methods
Compliance with Ethical Standards
This retrospective study was approved by the institutional review board of our institution (Samsung Medical Center 2021-05-009), and informed consent was obtained from patients before they underwent the biopsy procedures.
Patient Selection
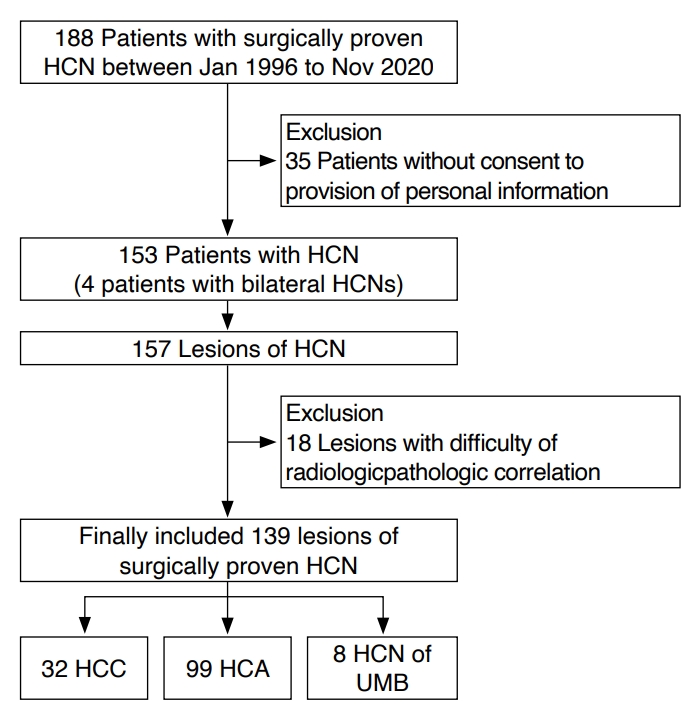
The study was conducted in patients with HCN (including HCA and HCC) according to surgical reports obtained from the authorsŌĆÖ institution between January 1996 and November 2020 (Fig. 1). A group of 188 patients was identified from this period of approximately 24 years. Among them, 157 lesions from 153 patients were included in the study after the exclusion of 35 patients who did not consent to the provision of personal information.
Furthermore, 18 patients were excluded due to difficulties in the radiologic-pathologic correlation resulting from the presence of multiple tumors or the absence of available US images. Finally, 139 cases in 135 HCN patients (31 men and 104 women; mean age┬▒standard deviation, 52.2┬▒12.8 years) who underwent surgical resection were enrolled in the study.
Ultrasonography
US was performed by one of 10 radiologists using high-resolution US equipment with 5-12 MHz linear array transducers. The entire thyroid gland and lateral neck compartments were analyzed throughout the examinations. The obtained images were retrospectively analyzed by two radiologists with 22 years and 3 years of experience, respectively.
In all cases, the following nine US characteristics and Korean-Thyroid Imaging Reporting and Data System (K-TIRADS) categories of the lesions were evaluated: tumor size, internal content, echogenicity, margin, orientation, shape, internal calcification, presence of a halo sign, and vascularity [20].
Tumor size was recorded as the longest diameter measured. The internal content of the mass was assessed as solid, predominantly solid (cystic portion Ōēż50%), predominantly cystic solid (cystic portion >50%), or cystic. The echogenicity was assessed in relation to the normal thyroid parenchyma and strap muscle. The margin of the mass was classified as smooth, spiculated/microlobulated, or ill-defined. The orientation was divided into parallel or nonparallel depending on whether the anteroposterior diameter was larger or smaller than the transverse or longitudinal diameter. Shapes were classified as irregular if the mass was neither round nor oval. Internal calcification was analyzed as follows: no calcification, microcalcification (echogenic foci Ōēż1 mm), macrocalcification (echogenic foci >1 mm), and rim calcification (peripheral curvilinear echogenic rim). The presence of a hypoechoic rim (halo sign) was also assessed. Lastly, the tumorŌĆÖs vascularity was classified as marked intranodular, mild intranodular, perinodular, none, or undetermined.
The target nodules had undergone at least one US-guided FNA or core needle biopsy (CNB) preoperatively. The first routine test for a thyroid nodule is typically FNA, but CNB was often carried out in patients with equivocal or nondiagnostic FNA results. Some nodules also underwent neither FNA nor CNB due to the presence of another primary tumor that required treatment, such as papillary thyroid carcinoma.
In FNA, the transducer was positioned vertically directly above the lesion, and a 23-gauge needle targeted the center of the lesion and was advanced using the freehand technique. While continuously verifying whether the needle tip was inside the lesion, mild negative pressure was applied to the syringe for effective aspiration. FNA was usually performed 1-2 times for each nodule at the authorsŌĆÖ institution. When a sufficient sample was obtained, it was smeared on a slide glass, fixed in 95% ethyl alcohol, and sent to the pathology department.
For CNB, an automatic biopsy system was used. After administering local anesthesia with lidocaine at the puncture site, the transducer was placed longitudinally so that the entire tract of the biopsy gun could be traced on US. Samples were obtained at least twice so that the lesion, the capsule of the lesion, and the normal thyroid parenchyma were all included [21]. At least two specimen cores were fixed in formalin and sent to the pathology department.
Pathological Examination
The pathologic diagnosis of HCNs was made by one of nine pathologists following World Health Organization criteria, followed by further division into three categories: HCA, HCC, and HCN of UMB [2,5]. The degrees of capsular invasion and vascular invasion were used to classify the specimens into these subtypes. The sizes and locations of the tumors were recorded. The tumor size was recorded based on the largest size relative to the long axis. Postoperative pathologic reports and pathologic tumor sizes were retrospectively analyzed to validate their concordance with the measurements made on US.
Statistical Analysis
The US characteristics of the lesions were assessed according to the pathologic subtypes. The significance of the difference between the US-measured tumor size and the pathologic tumor size measured using the surgical specimen was assessed. The Shapiro-Wilk test was conducted to verify the normality assumption. If the normality assumption was satisfied, the paired t-test was performed; if not, the Wilcoxon signed rank test was used. For cases of surgically confirmed HCN, the Pearson chi-square test was carried out to determine whether there was a significant difference in the distribution of lesions of Bethesda category 4 or higher as surgical candidates in the CNB and FNA groups. Logistic regression analysis was conducted to explore the association between clinical and US features and the benign and malignant nature of HCNs. All factors with P<0.05 in the univariate analysis were included in multiple logistic regression. A receiver operating characteristics curve analysis was conducted, and the area under the curve was estimated to evaluate the ability of US tumor size to predict malignancy. The best cutoff for US tumor size to distinguish HCCs from HCAs was determined.
Results
Of the 139 HCNs, the final pathology examinations found 99 (71.2%) HCAs, 32 (23.0%) HCCs, and eight (5.8%) HCNs of UMB. The clinical and radiologic features of HCN along with their final pathology results are presented in Table 1. On US, HCNs commonly presented as solid (76.3%), oval to round (100%), hypoechoic (70.5%) masses, with a smooth margin (95.0%) and a halo sign (90.6%), as well as an absence of internal calcification (93.5%). HCCs were significantly larger than HCAs (mean┬▒standard deviation, 3.4┬▒1.6 cm vs. 2.2┬▒1.2 cm; P<0.001).
Table 2 shows the distribution of HCAs, HCCs, and HCNs of UMB according to the test modality (FNA/CNB) and Bethesda categories. Most of the cases belonged to Bethesda III or IV, while only six of 119 cases (5.0%) belonged to Bethesda V or VI when excluding cases that did not undergo biopsy due to any other coexisting malignancy. There were also no cases diagnosed as Bethesda V or VI in masses that underwent CNB.
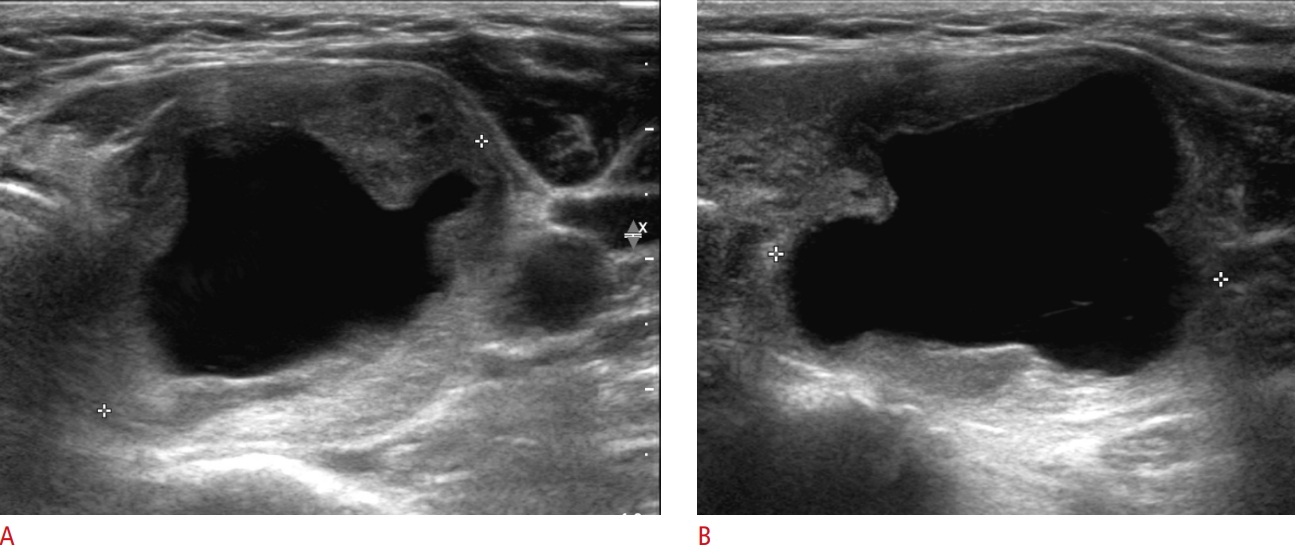
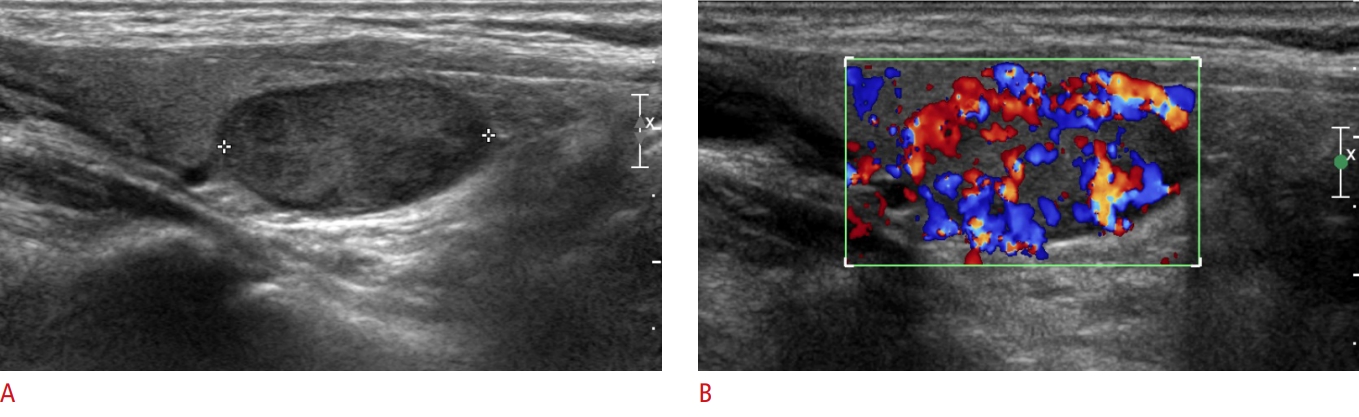
The univariate analysis, as shown in Table 3, showed that three features were significantly associated with HCA versus HCC: internal content (P=0.019), US tumor size (P<0.001), and pathologic tumor size (P<0.001). HCC masses more frequently showed cystic changes than HCAs (38%, 12/32 vs. 17%, 17/99, respectively; P<0.001) (Fig. 2). Other factors such as echogenicity, margin, orientation, calcification, the halo sign, vascularity, K-TIRADS category, and Bethesda category did not show statistical significance for differentiating HCC from HCA. The multiple logistic regression analysis, as presented in Table 4, revealed that the US tumor size was an independent significant predictor of malignancy (P=0.001; odds ratio, 1.730 for each 1-cm increase [95% confidence interval, 1.258 to 2.375]) (Fig. 3). The best cutoff value of US tumor size for predicting malignancy was 3.35 cm (sensitivity, 53.1%; specificity, 87.9%). Table 5 presents the diagnostic performance according to variable US tumor size cutoff values for predicting malignant HCNs (HCCs).
HCNs were commonly smaller when pathologically measured using surgical specimens than when measured by US (smaller, same, and greater than US measurements in 60.4%, 21.6%, and 18.0% of cases, respectively; P<0.001). Furthermore, 12% of HCNs showed a more than 30% smaller size after surgery compared to the preoperative tumor size. There was no significant difference in the magnitude of the size discrepancy between the HCC group and the HCA group.
Discussion
Previous studies have reported that 5% to 35% of HCNs are malignant [22-24]. In the present study, 23% of all HCN cases were identified as malignancies. Although timely surgical treatment is essential, it remains challenging to reliably distinguish malignant from benign HCNs in preoperative settings [3]. For this reason, surgeons may have difficulty deciding when to operate on a thyroid nodule suspected of HCN on FNA or CNB, and whether to perform lobectomy or total thyroidectomy.
Researchers have investigated factors that can predict the malignant potential of HCNs preoperatively to aid the surgeonŌĆÖs clinical decision process, including the extent of surgery. In particular, there have been many studies of clinical factors such as age, sex, and tumor size; malignant potential increases in male patients who are older and have a larger tumor size [18,25].
However, it is difficult to predict HCC even with the current K-TIRADS. Factors such as echogenicity, margin, and internal calcification are known to be insignificant for predicting malignant potential in HCNs [18]. Tumor size is the most significant factor in predicting malignant potential, and its cutoff was reported to range from 1.5 to 4.0 cm [13,17,18,26]. In this study, US tumor size was found to be a significant predictor of malignancy in HCNs, with a preoperative US tumor size >3.35 cm as the best cutoff to distinguish malignant from benign HCNs. Each US and pathologic tumor size used to predict malignancy showed meaningful results in the univariate analysis. However, as the pathologic tumor size cannot be known before surgery, the US tumor size, which can be obtained preliminarily, is more useful for preoperative planning.
To the best of the authorsŌĆÖ knowledge, this is the first study to identify the possibility that cystic changes detected on US may be a significant factor in predicting the malignancy of HCNs using univariate regression analysis. As the solidity of nodules decreases, the degree of suspicion for malignancy also becomes lower [27]. However, HCNs did not follow this theory in the present study, which may be due to the fact that carcinomas are generally larger than adenomas and thus have a higher probability of hyaline degeneration or internal hemorrhage/infarction. Due to the small number of HCNs with cystic changes, statistical significance was not reached in the multivariate analysis.
In this study, cystic changes on US in HCNs were shown to be related to histology. These changes often lead to size discrepancies between US and pathology. No significant difference was found in the magnitude of the size reduction between the HCC group and the HCA group. Several studies have reported that thyroid nodules (including HCN) may undergo necrosis or infarction after traumatic procedures, such as FNA or CNB [28,29]. Microvascular supply inhibition or vascular supply compromise due to tissue loss and the intrinsic energy deficiency of oncocytic cells have been suggested as causes, and the size of tumors may decrease through hemorrhage and fibrosis [29-31].
This study had several limitations. First, this was a retrospective study. However, due to the rarity of HCNs, a retrospective approach to surgically confirmed cases was unavoidable. Second, the findings were not compared between HCN and other histologic categories. Third, the data was collected over a 20-year period, for which reason the US images may have been heterogeneous.
In conclusion, US tumor size was identified as an independent predictor of malignancy in HCNs, and a US tumor size >3.35 cm might be used as a criterion to suggest malignancy. The size of HCNs often showed discrepancies between US and pathologic measurements.
 Download Citation
Download Citation PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Full text via PMC
Full text via PMC



