

 Print
Print facebook
facebook twitter
twitter Linkedin
Linkedin google+
google+

Introduction
Gastric submucosal tumors (SMTs) are occasionally found during routine gastroduodenoscopy (prevalence, 0.2%–3%) [1], most of which are gastrointestinal stromal tumors (GISTs) and leiomyomas. Based on the newly published European Society of Gastrointestinal Endoscopy (ESGE) guideline, the indications for the treatment of SMTs are as follows: risk of malignancy (GISTs, neuroendocrine neoplasms, and granular cell tumors); symptoms such as obstructions or bleeding; and lesions in specific locations for patients receiving bariatric surgery [2]. If there is an indication for resection, the ESGE suggests endoscopic resection (ER) as an alternative to laparoscopic surgery for gastric GISTs <35 mm in size that protrude into the gastric lumen. ER, which includes endoscopic submucosal excavation (ESE), endoscopic full-thickness resection (EFTR), and submucosal tunneling endoscopic resection (STER), can be performed to curatively resect tumors in an en bloc fashion [3,4], with a high R0 resection rate, a low serious complication rate, and a low recurrence rate [2].
The pooled estimate rate of delayed perforation was reported to be 0.14%–5.78%, and the pooled rate of delayed bleeding was 0.14%–1.01% [5,6]. ESE is an endoscopic submucosal dissection (ESD)–derived technology, and it is more suitable for the ER of SMTs originating from the muscularis propria (MP) [7]. For SMTs involving the serosa and extraluminal component, another ESD-derived technology known as EFTR is applied [8-10]. Although both of these procedures can curatively resect tumors in an en bloc fashion, perforation seems to result in more problems. Compared with EFTR, ESE tends to have advantages of earlier postoperative feeding, shorter postoperative hospital stays, lower hospitalization expenses, and a lower probability of infection [8,11]. Hence, attempts should be made to avoid perforation during ER if the circumstances are appropriate. Being able to predict the risk of perforation would help endoscopists be more cautious and be prepared ahead of time; moreover, appropriate patients could be selected for inexperienced endoscopists.
Endoscopic ultrasonography (EUS) is an important technique in the diagnosis of SMTs, as it can provide information on the layer from which the SMTs originate, as well as the size, borderline, and echoes to help evaluate the possible pathology of the SMTs [12]. Additionally, it can show information on the membrane integrity, spatial relationship between the tumor capsule and the serosal layer, and other factors that predict procedural complications and patients’ prognoses [13]. Zhang et al. [13] showed that SMTs located in the superficial MP with a length of the muscular connection <40% of the tumor capsular semi-circumference may have a lower risk for perforation.
In real-world clinical practice, it is sometimes difficult to differentiate the superficial and deep MP, due to a lack of a quantification index and the fact that the length of the connection is hard to measure, as it is usually a curved line rather than a straight line. The authors agree with the above-mentioned researchers that a deeper location of the SMT is associated with a higher risk of perforation, and a quantification index would help prove this hypothesis. Therefore, this study was conducted to determine important parameters in EUS images to predict perforation and to attempt to build predictive models to guide clinical practice.
Materials and Methods
Compliance with Ethical Standards
The study protocol was approved by the Institutional Review Board of the Sixth Affiliated Hospital, Sun Yat-sen University (approval code: 2021ZSLYEC-060). The requirement for informed consent from human subjects was waived by the Institutional Review Board.
Patients
Consecutive patients with gastric SMTs originating from MP who received ER in the authors’ affiliated hospital from May 1, 2013 to January 15, 2021 were retrospectively reviewed. The criteria for resection of SMTs were as follows: a risk of malignancy, symptoms such as obstructions or bleeding, and an eagerness to resect the tumor from the patients (rather than surveillance). The inclusion criteria were as follows: (1) EUS was performed in the authors’ affiliated hospital, and EUS images could be obtained; (2) gastric SMTs were confirmed by using EUS; (3) SMTs originated from the MP; and (4) ER was performed in the authors’ affiliated hospital. The exclusion criteria were as follows: (1) failure of ER due to comorbidities; (2) use of band ligation; (3) use of both ER and laparoscopic resection at the start of the treatment (except for cases in which ER failed, followed by conversion to laparoscopic surgery); and (4) use of STER. The patients were classified into two groups based on whether they had perforation (the case group), or not (the control group). Perforation was defined as endoscopically visible perforation during the ER procedure, EFTR, or if perforation was not noticed during ER but was confirmed by using computed tomography (CT) or X-ray results after the procedure (Fig. 1 shows the EUS and ER images of typical cases with or without perforation).
Endoscopic Equipment
The machines used to perform EUS were EU-ME1 (Olympus, Tokyo, Japan), MAJ-1720 (Olympus), SU-9000 (Fujifilm, Tokyo, Japan), SP-900 (Fujifilm). The ultrasonic endoscopes or ultrasound probes used were GF-UE260-AL5 (Olympus), GF-UCT240-AL5 (Olympus), UM-2R (Olympus), UM-3R (Olympus), EG-530UT2 (Fujifilm), EG-580UT (Fujifilm), EG-580U (Fujifilm), P2612-M, and P2615-M. (Fujifilm). The EUS procedure was performed via the water immersion method, balloon assistance, or both methods at distinct times. The frequency used for GF-UE260-AL5, GF-UCT240-AL5, EG-530UT2, EG-580UT, and EG-580U was 7.5 MHz or 12 MHz; the frequency for UM-2R or UM-3R was 20 MHz; the frequency for P2612-M was 12 MHz, and the frequency for P2615-M was 15 MHz.
ER Procedure
The endoscopists who performed the ER procedures were divided into two groups based on their experience (experienced endoscopists were defined as those with experience of more than 25 cases every year for gastric SMTs, and inexperienced endoscopists were those with experiences of no more than 25 cases). Some patients were treated under intravenous anesthesia by using propofol with airway intubation, whereas other patients were sedated with midazolam and dezocine. In both situations, heart rate, blood pressure, and oxygen saturation were monitored. Gastroduodenoscopy (GIF-Q260J or GIF-HQ290, Olympus) was used during the procedures. A short, transparent cap (Olympus) was attached to the tip of the endoscope to improve visualization to facilitate resection. A dual-knife (KD-655L/KD-655Q, Olympus), IT-knife (KD-611, Olympus), hook-knife (KD-620LR, Olympus), or combinations thereof were used to dissect the submucosal layer and to peel the tumor. Other equipment that was used included injection needles (ET2522-C4, ENDO-FLEX GmbH, Voerde, Germany), snares (NOE342216-C, ENDO-FLEX GmbH), high-frequency hemostatic forceps (FD-410LR, Olympus), and hemoclips.
ER was performed in the following manner [3]: first, marker dots were made by using electrocoagulation close to the lesion; subsequently, methylene blue solution (several milliliters) was injected around the lesion by using the injection needle to lift the mucosa off (in some procedures, this step was omitted). The mucosa was incised along the marker dots by using the dual-knife or hook-knife, and the MP layer was peeled along the capsule of the lesions with a dual-knife, IT-knife, hook-knife, or a combination of the knives. After the resection of the tumors, exposed vessels on the wound surface were coagulated via dual-knife or high-frequency hemostatic forceps to prevent delayed bleeding, and clips were placed (or a purse-string suture was performed) to prevent delayed bleeding or perforation [14]. If perforation occurred in the procedure, then a circumferential incision was made surrounding the lesion by using a dual-knife, IT-knife, or hook-knife. The gastric wall defect was then closed by placing clips or by making purse-string sutures. If pneumoperitoneum occurred, a 20-gauge needle was inserted into the right lower quadrant of the abdomen to decompress the abdominal cavity. A nasogastric tube was then inserted after ER for those cases who had perforation during the procedure.
Pathology Diagnosis
All of the resected specimens were fixed in 10% buffered formalin, embedded with paraffin, sectioned into slides, and stained with hematoxylin and eosin, as well as several immunohistochemical stains (Dog1, alpha-SMA, c-Kit, CD34, desmin, actin, S-100, and other stains). A GIST was diagnosed based on the presence of spindle or epithelioid cells with positive c-Kit, CD34, and Dog1 staining; additionally, leiomyoma or leiomyosarcoma was diagnosed based on positive actin staining, and schwannoma was diagnosed based on positive S-100 staining.
Data Collection
Patients’ electronic medical records were reviewed to obtain the following data: age, sex, height, weight, medical history, laboratory tests (routine blood tests, serum albumin [ALB], and carcinoembryonic antigen), imaging results (abdominal CT, EUS findings [the origin, location, and size of the SMT] and the EUS images), gastroscopy findings (the procedure records of ER including procedure time, endoscopists, incidences of perforation, and incidences of en bloc resection), pathology results, final diagnosis, postoperative complications, and other data.
Measurements and Outcome Parameters
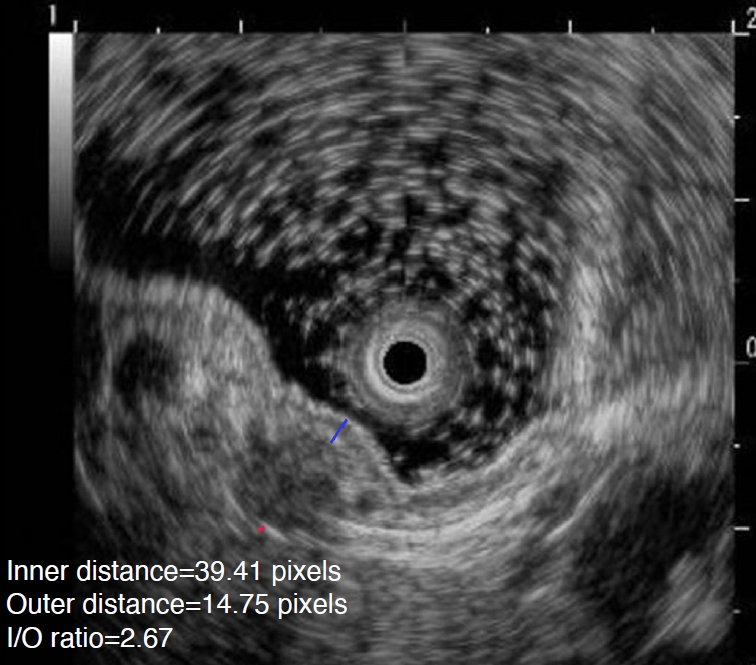
To evaluate the depth of the SMT that was located using a quantification index, we developed a parameter known as the ratio of inner distance to the outer distance (I/O ratio). First, we reviewed the EUS images of the patients, and selected one case with the maximum cross-sectional axis of the SMT. Afterwards, two experienced endoscopists (with experience involving more than 200 cases of EUS) discussed and selected the points of the SMT with the most prominent protrusions to the mucosal surface and serosal surface, respectively. If the two endoscopists could not agree with each other, then a third experienced endoscopist evaluated the data. Third, after the two points were determined, Adobe Photoshop CS6 version 13.0×64 (the Ruler tool) was used to measure their distance to the mucosal surface (inner distance) and serosal surface (outer distance) (Fig. 2 shows what the inner distance and outer distance represents); to minimize the measurement error, we measured each distance five times and then eliminated the smallest and largest values. The average value of the remaining three values was regarded as the final distance. Finally, the ratio of the inner distance and the outer distance was calculated, which was represented by the I/O ratio. The endoscopists who selected the images, discussed and selected the points, and measured the I/O were all blinded to whether the images were in the case or the control groups.
The primary outcome parameter was to build models to predict the risk of perforation and to evaluate its accuracy. The secondary outcome parameters included differences between the case and control groups in the EUS findings (the origin, location, size, and I/O ratio of the SMTs).
Statistical Analysis
SPSS version 22 (IBM Corp., Armonk, NY, USA) was used to perform the statistical analyses. As none of the continuous variables in this study had a normal distribution, they were expressed as the median (range) and tested using the nonparametric Mann-Whitney U test. Categorical variables were expressed as numbers (percentages) and tested using the chi-square test. Univariate analysis was first performed, and variables with a P-value <0.1 or that were of interest were included in the logistic multivariate analysis (the forward logistic regression model was chosen). The regression equation (predictive model) was obtained, the regression coefficients were regarded as the weights for the respective variables, and a predictive value for each patient was calculated. MedCalc version 15.2.2 (MedCalc Software bvba, Ostend, Belgium; http://www.medcalc.org; 2015) was used to draw the receiver operating characteristic (ROC) curve for the use of the predictive values to assess the ability of the model and to identify the optimal cutoff value (with the maximum Youden index) for predicting perforation. The area under the ROC curve (AUC), sensitivity, specificity, positive likelihood ratio (PLR), negative likelihood ratio (NLR), and their 95% confidence intervals (CIs) were also calculated. Statistical significance was defined as P<0.05 (two-tailed).
Results
Baseline Characteristics of Patients
From May 1, 2013, to January 15, 2021, 692 EUS procedures were confirmed to have gastric SMTs originating from the MP, and 199 EUS procedures (194 patients, with five patients having two SMTs, and each SMT being regarded as a separate EUS procedure for the analysis) were finally chosen for analysis. Fig. 3 shows the selection algorithm.
The median age of the patients was 53 years old (range, 19 to 81 years), and 88 (44.22%) of them were men. The two groups had no significant difference in sex, body mass index, or history of hypertension or diabetes. Among the laboratory tests, the ALB level seemed to be higher in the control group (P=0.040).
Endoscopic Characteristics and EUS Findings
The median value of the long axis and short axis of the tumor was 1 cm (range, 0.3 to 5 cm) and 0.8 cm (range, 0.3 to 4 cm), respectively, with no significant difference between the two groups. A total of 30.65% of the SMTs mainly grew intraluminally; additionally, 12.06% of the SMTs mainly grew extraluminally, and 57.29% of the SMTs mainly grew both intraluminally and extraluminally. The two groups showed no difference in the growth pattern. The median I/O ratio of the patients was 1.79 (range, 0.31 to 6.24), and the ratio was higher in the case group (P<0.001). The baseline and endoscopic characteristics of the patients are shown in Table 1.
Clinical Outcomes of ER
During ER, 82.91% of the procedures were performed under sedation, and 17.09% of the procedures were under general anesthesia, with no significant difference between the two groups (P=0.730). Five patients (2.51%) experienced technical failure of the ER procedure (all of the patients were in the case group). In one patient, the tumor was too large, and it was partially resected in the first ER procedure; several days later, the tumor was successfully resected in the second ER procedure. In the second patient, the tumor fell into the abdominal cavity after resection by endoscopy, and it was retrieved using laparoscopic surgery. In the third patient, there were difficulties with handling the perforation after resection of the tumor, and a decision was made to perform laparoscopic surgery. The fourth patient did not cooperate well after the perforation and was finally transferred to the operating room; the tumor was then en bloc resected under general anesthesia. For the last patient, the tumor could not be found during the procedure. The clinical outcomes of the patients are shown in Table 2.
The en bloc resection rate was 96.48%, with no difference between the two groups (P>0.99). ER lasted for a median of 73 minutes (range, 22 to 543 minutes), and it was longer in the case group (P=0.016). Twenty-one patients (21.21%) in the case group had abdominocentesis during ER. A total of 66.83% of the procedures used injections, and 98.9% of the procedures were performed by experienced endoscopists, with no significant difference between the two groups.
Univariate and Multivariate Analysis
The univariate analysis showed that age, SMT located in the gastric fundus, the I/O ratio, and the pathology of the SMT were potential risk factors for predicting perforation (Table 3). The multivariate binary logistic analysis further proved that age, the I/O ratio, and the pathology were predictive model parameters. However, most of the time, it was not possible to identify the pathology results of the SMT before ER; thus, two models were built that differed in terms of whether pathology was included as a parameter: model 1 included pathology, and model 2 did not. Table 4 shows the multivariate analysis results of the two models. The predictive value in model 1 was: 1/[1+e-(-5.740+0.036*Age+1.005*I/O ratio+2.396*GIST+2.71*others)], and the predictive value in model 2 was: 1/[1+e-(-4.097+0.045*Age+0.864*I/O ratio)].
The AUCs of model 1 and model 2 were 0.836 (95% CI, 0.778 to 0.885; P<0.001) and 0.755 (95% CI, 0.689 to 0.813; P<0.001), respectively (Fig. 4 shows the ROC curves of the predictive ability of the two models). In model 1, if 0.64479 was used as the cutoff point, the sensitivity was 64.7% (95% CI, 54.4% to 74.0%), the specificity was 90.0% (95% CI, 82.4% to 95.1%), the PLR was 6.46 (95% CI, 3.50 to 11.80), the NLR was 0.39 (95% CI, 0.30 to 0.50), and the accuracy rate was 77.39%. In model 2, if 0.49665 was the cutoff point, the sensitivity was 69.7% (95% CI, 59.6% to 78.5%), the specificity was 76.0% (95% CI, 66.4% to 84.0%), the PLR was 2.90 (95% CI, 2.00 to 4.20), the NLR was 0.40 (95% CI, 0.30 to 0.50), and the accuracy rate was 72.86%.
Discussion
In this study, the patients in the case group tended to be older, have lower ALB levels, have SMTs more commonly located at the gastric fundus, have a higher I/O ratio, and have a higher proportion of GISTs or schwannomas. The multivariate analysis further helped in building two models to predict perforation, and the AUCs of model 1 and model 2 were 0.836 and 0.755, respectively.
In the case group, a certain proportion (21.21%) of patients had abdominocentesis during ER; these data have not been published in previous studies, thus indicating the importance of avoiding perforation if the situation is appropriate. A literature search demonstrated that there was still a lack of articles investigating risk factors using EUS images to predict perforation. Zhang et al. analyzed 43 patients and found that more SMTs in the perforation group were located in the deep MP and had a length of the muscular connection ≥40% of the tumor capsular semi-circumference; however, they did not perform univariate or multivariate analyses [13]. Moreover, it was difficult to apply their findings in realistic situations. The authors’ experiences supported the proposal that deeper SMTs have a higher risk of perforation; hence, this study developed a new parameter known as the I/O ratio. The reason for the use of this ratio is that this was a retrospective study, meaning that it was not possible to know the absolute distance; however, it was possible to measure the relative distance, so the ratio was adopted, with a larger ratio indicating a deeper SMT. For the first time, these results proved that the I/O ratio was much higher in the case group, and the univariate and multivariate analyses further supported that the I/O ratio was a risk factor for perforation. This phenomenon is considered reasonable, as a deeper tumor location means that deeper layers were cut, and the higher chance it had to be perforated in ER.
Age was another risk factor for perforation and was selected as a parameter in the model in this study. However, in previous studies, the researchers thought that age was not a risk factor for perforation, but was a possible risk factor for delayed bleeding [15,16]. The reason for this phenomenon may be that the present study regarded age as a continuous variable and did not divide the patients into different age groups, whereas in previous studies, the researchers classified the patients into different age groups. The reason why age was a risk factor for perforation was unknown, although a possible explanation is that older patients were more likely to have comorbid hypertension or other diseases involving vascular sclerosis.
The univariate analysis showed that SMTs located at the gastric fundus were also a risk factor for perforation. Previous studies have supported the idea that tumors located at the upper portion of the stomach were more likely to be perforated [17,18]. There may be several reasons for this. First, it was difficult to reach the fundus due to retroflexion of the endoscope. Second, the knife was vertically oriented to the fundus, which could also result in a prolonged procedure. Third, the gastric fundus is thinner than other parts of the stomach. Fourth, the submucosal arteries were larger in the upper stomach, and intraoperative bleeding may have impaired the field of view during ER [3,19-21]. Moreover, tumors located at the upper portion of the stomach were reported to be associated with incomplete resection [18]; additionally, the spleen and many blood vessels surrounding the gastric fundus increased the risk of other complications [3]. Hence, it was suggested that only experienced endoscopists should perform such procedures [3].
Another interesting finding of this study is that the pathology of the tumors was a risk factor for perforation, as leiomyoma was a protective factor, whereas GIST and schwannoma were risk factors. A reason for this phenomenon may be that, compared with other tumors, leiomyoma was softer, with greater elasticity and better compliance, whereas GIST and schwannoma were relatively harder and were more likely to be perforated. These results were slightly different from a previous study [13], as those researchers showed no difference for perforation regarding pathology; however, in their study, their sample size was smaller than that in this study. Moreover, Hsu et al. [22] showed that ESD procedures tended to be more likely to involve complications (perforation, delayed bleeding, and surgical interventions) for GISTs than for leiomyomas, which was in accordance with the present results in some ways. The predictive models were constructed with consideration of the fact that it was often not possible to know the pathology result of the SMT before ER; therefore, two models were built, differing in terms of whether pathology was included or not. If the pathology of the SMT is known, model 1 could be used. Of note, a study showed that artificial intelligence (AI) technology could help in differentiating GISTs and non-GISTs [23], especially for cases with sizes ≥20 mm. However, at the present time, the technology of AI has not been widely used in clinical practice; thus, if the pathology is not known in advance, model 2 could be used to make a prediction.
This study had some limitations. First, this was a single-centered study, and the predictive models that were built were not tested in other centers; external validation would be needed to apply the models to other centers. Second, this was a retrospective study, and some information was lacking; for example, the absolute distance of the tumor edge to the mucous layer and serosal layer may also be important factors, but it was not possible to evaluate this factor in the present study. Hence, a well-designed prospective study would be better for the assessment of inner and outer distances. Third, most of the tumors in this study were smaller than 20 mm, which has been reported to be a risk factor for perforation in gastric ESD in other studies [21,24]; thus, this factor was not regarded as an important parameter in the model. The inclusion of more patients with SMTs >20 mm could possibly enable a better model to be built. Fourth, the I/O ratio was measured in this study, although the distance may be influenced by several factors. For example, if the balloon-assisted method was used, the thickness of the layer seemed to change depending on the degree of pressing against the lesion, and if the tumor was adjacent to the liver or the spleen, their thickness would also be influenced. Additionally, various endoscopes and probes were used in this study, which could possibly influence the results; however, as both the inner distance and outer distance would be influenced, calculating their ratio might attenuate the impact of this issue. Thus, caution is warranted in these situations when using this method. Fifth, the function of EUS images in predicting perforation was evaluated in a preliminary sense, and the AUC values of model 1 and model 2 were only 0.836 and 0.755, respectively. However, both of these values were >0.7, which was not optimal, and models with greater AUC, sensitivity, and specificity are still needed.
In conclusion, EUS was useful in predicting perforation of ER for gastric SMTs originating from the MP, and the I/O ratio was an important factor. In addition, age, tumors located in the gastric fundus, and tumor pathology of GISTs or schwannomas were also possible risk factors. Overall, this study developed two models for predicting perforation, which may serve as a useful tool in clinical practice.



 Download Citation
Download Citation PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI



