

 Print
Print facebook
facebook twitter
twitter Linkedin
Linkedin google+
google+

Introduction
Ultrasonography (US) is the primary tool used to evaluate thyroid nodules and their malignancy risk, and to identify patients who require fine-needle aspiration (FNA) or core needle biopsy (CNB) [1]. Many international societies have proposed risk stratification systems (RSSs) for the clinical management of thyroid nodules. Most of these systems stratify malignancy risk based on US features such as composition, echogenicity, punctate echogenic foci (microcalcifications), nonparallel orientation (taller-than-wide shape), and irregular (microlobulated/spiculated) margin [2-7].
Although US-based RSSs have been increasingly used for the diagnosis and management of thyroid nodules [2-7], each RSS incorporates different definitions for the US lexicon that describes solid composition [8]. The 2021 Korean Thyroid Imaging Reporting and Data System (K-TIRADS) [5] defines solid nodules as those for which an obvious cystic component is not visualized, whereas the American College of Radiology (ACR)-TIRADS [6] defines solid nodules as nodules that contain small cystic components occupying no more than approximately 5% of the overall volume. The European (EU)-TIRADS [7] defines solid nodules as nodules composed almost entirely of soft tissue with <10% liquid. The American Thyroid Association (ATA) [3] and American Association of Clinical Endocrinologists/American College of Endocrinology/Associazione Medici Endocrinologi (AACE/ACE/AME) do not clearly specify definitions of composition [4]. These differences in definition could affect the overall diagnostic performance of US-based RSSs. Thus, appropriate US-based definitions for solid composition need to be standardized for thyroid nodules by assessing the malignancy risk of minimally cystic thyroid nodules (MCTNs).
A previous study [9] that evaluated the malignancy risk of MCTNs defined MCTNs as nodules with a cystic portion Ōēż10% compared with purely solid or partially cystic thyroid nodules (PCTNs). MCTNs showed a low risk of malignancy (3.3%), similar to PCTNs, regardless of echogenicity or the presence of suspicious US features [9]. To the best of the authorsŌĆÖ knowledge, however, no multicenter study has reported the malignancy risk of MCTNs. Therefore, the aim of this multicenter study was to investigate the malignancy risk of MCTNs using cyto-histopathologic diagnoses.
Materials and Methods
Compliance with Ethical Standards
The institutional review boards of 26 different hospitals approved this study, and the requirement for informed patient consent was waived because of its retrospective nature.
Study Population
Patient data were collected from the 26 hospitals (Thyroid Imaging Network Korea, THINK). Consecutive patients who underwent thyroid US between June 2015 and September 2015 were enrolled in this study: Patients who had nodules Ōēź1 cm and had undergone FNA, CNB, or surgery for nodules were included. Patients were excluded from the study if the thyroid nodule was smaller than 1 cm, there was no reference standard test (biopsy or surgery), or the image quality was suboptimal. Among 22,775 consecutive patients who had undergone thyroid US at 26 institutions, 16,679 patients were excluded due to a thyroid nodule size less than 1 cm (n=12,130), no reference standard test (biopsy or surgery) (n=4,304), or suboptimal image quality (n=245). Among them, 1,015 patients with 1,102 nodules were further excluded because of inconclusive biopsy results. Furthermore, 107 nodules were excluded because the US characteristics could not be analyzed in 59 isolated macrocalcifications (entirely calcified nodules) and 48 purely cystic nodules (Fig. 1).
Ultimately, 5,601 thyroid nodules in 4,989 consecutive patients (4,101 women, 888 men; mean age, 53.3┬▒12.7 years; age range, 19 to 93 years) were included. Among the 5,601 nodules, 1,089 were finally diagnosed as malignant based on histopathological results after surgery (n=927, 85.1%) or malignant FNA or CNB diagnoses (n=162, 14.9%). The other 4,512 nodules were finally diagnosed as benign nodules based on cyto-histopathology after surgery (n=390, 8.6%), at least two benign diagnoses via FNA or CNB (n=594, 13.2%), or one benign diagnosis based on FNA or CNB that did not show follicular neoplasm, suspicious malignant, or malignant biopsy results in the initial or repeat FNA or CNB (n=3,528, 78.2%).
US Examination and Nodule Classification
Real-time US was performed with a high-resolution ultrasound scanner that was equipped with a 5ŌĆō12 MHz or an 8ŌĆō15 MHz linear probe. The scanning protocol included both transverse and longitudinal images of the thyroid nodules, using representative Digital Imaging and Communications in Medicine (DICOM) images. To establish a baseline consensus regarding the US lexicon of thyroid nodules, two consensus meetings were held prior to this study. Seventeen experienced radiologists (with 8ŌĆō22 years of experience with thyroid US) participated to reach a consensus on the definitions of the US features to be analyzed.
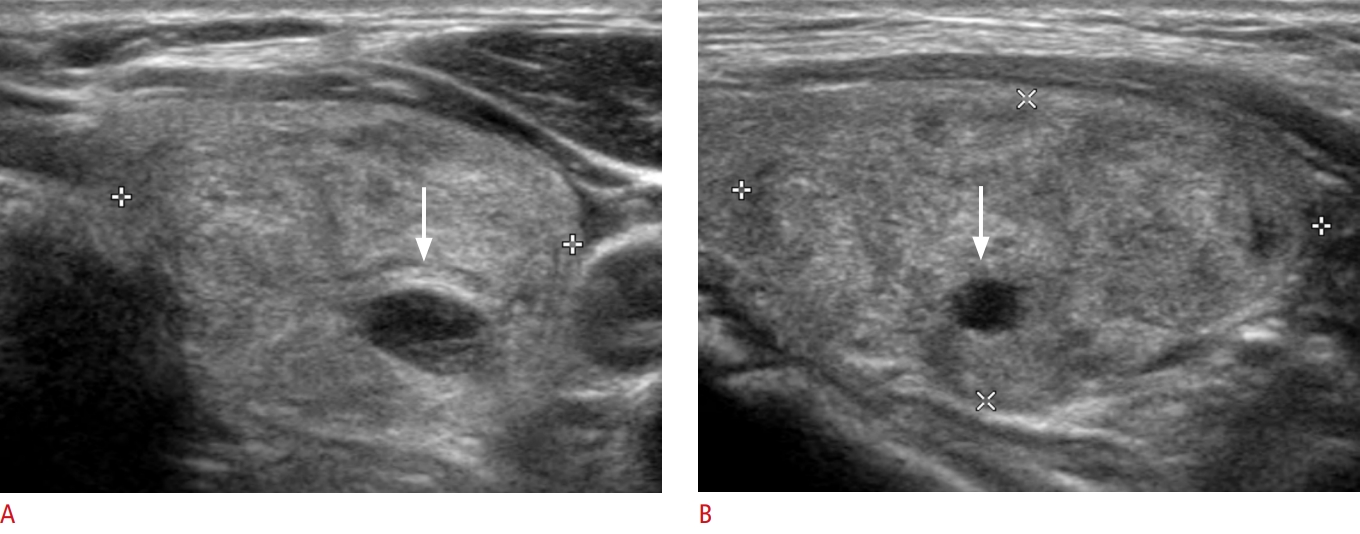
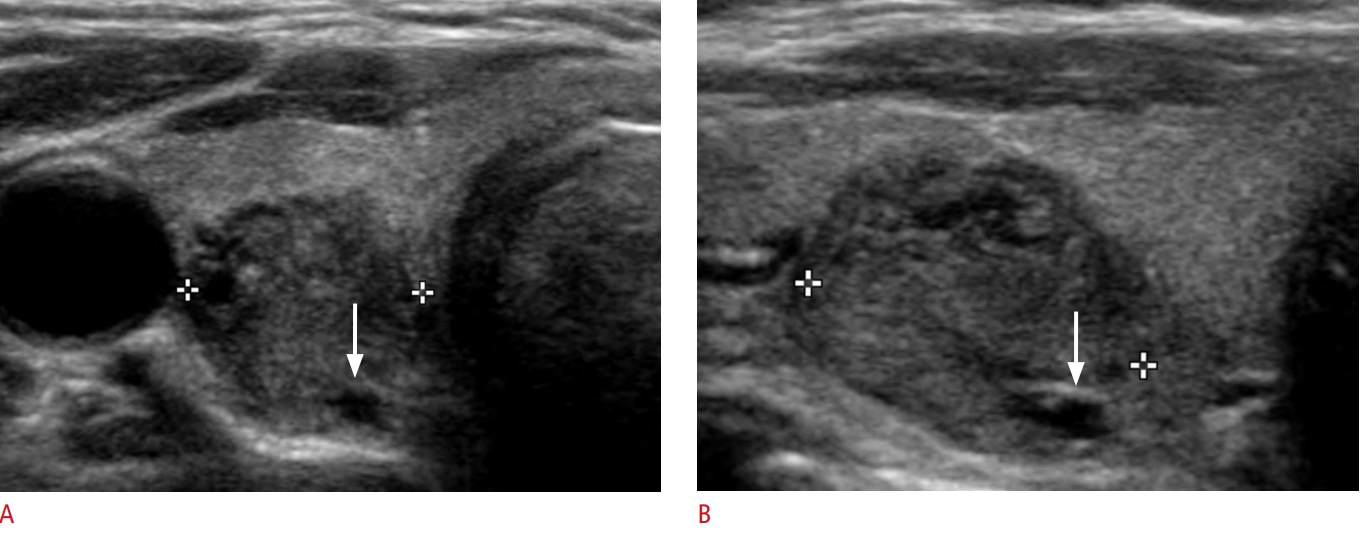
In this study, US images were analyzed in DICOM format using an online program (AIM AiCRO; https://study.aim-aicro.com). Seventeen experienced radiologists, who were blinded to histopathologic findings and the final diagnoses, retrospectively analyzed the US features of each thyroid nodule according to the revised 2021 K-TIRADS lexicon for composition, echogenicity, orientation (shape), margin, and echogenic foci (calcifications) [5]. The composition of each thyroid nodule was defined according to the percentage of the cystic portion in the entire nodule: purely solid (no cystic portion), MCTNs (cystic portion Ōēż10%), and PCTNs (predominantly cystic or predominantly solid nodules with any cystic portion >10%) (Fig. 2). Vessels, marked hypoechogenicity of the solid portion, fibrosis, or shadowing artifacts were carefully distinguished from minimally cystic changes. Nodule echogenicity was categorized into hypoechogenicity (marked or mild hypoechogenicity) or isohyperechogenicity based on the relative echogenicity of the nodule compared with the normal thyroid parenchyma and the anterior neck muscles (Fig. 3). Punctate echogenic foci (microcalcifications), nonparallel orientation (taller-than-wide shape), and irregular (microlobulated/spiculated) margin were defined as suspicious US features [5,10].
Statistical Analysis
The malignancy risk of MCTNs was evaluated in all nodules and subgroups based on composition, size, echogenicity and the presence of suspicious US features (punctate echogenic foci, nonparallel orientation, and irregular margin). The chi-square test or Fisher exact test was used to compare malignancy risk according to nodule composition in all nodules and according to echogenicity and the presence of suspicious US features in subgroups. All statistical analyses were conducted using SPSS for Windows (version 24.0, IBM Corp., Armonk, NY, USA). A P-value <0.05 was considered to indicate statistical significance.
Results
Nodule Characteristics
The demographic characteristics of 5,601 nodules in 4,989 patients are presented in Table 1. The final diagnoses of the malignant nodules included 989 papillary thyroid carcinomas (90.8%) and 100 other malignant tumors (9.2%), which comprised 62 follicular carcinomas (5.7%), 12 medullary carcinomas (1.1%), seven poorly differentiated carcinomas (0.6%), six anaplastic carcinomas (0.6%), five metastases (0.5%), four unspecified malignancies (0.4%), three lymphomas (0.3%), and one squamous cell carcinoma (0.1%).
Overall Malignancy Risk of Thyroid Nodules According to Composition
Table 2 lists the frequency and malignancy risk of 5,601 thyroid nodules according to their composition. The frequency of purely solid nodules, MCTNs, and PCTNs was 3,041 (54.3%), 1,259 (22.5%), and 1,301 (23.2%), respectively. MCTNs were more prevalent in benign nodules than malignant nodules (P<0.001). The overall malignancy risk of MCTNs was 8.8%, which was significantly lower than that of purely solid nodules (29.5%) (P<0.001) and slightly higher than that of PCTNs (6.2%) (P=0.013).
Malignancy Risk of Thyroid Nodules According to Composition and Echogenicity
Table 3 shows the frequency and malignancy risk of thyroid nodules according to their composition and echogenicity. MCTNs were found in 12.4% (249/2,014) of the hypoechoic nodule group and 28.2% (1,010/3,587) of the isohyperechoic nodule group. MCTNs were more prevalent in benign nodules than in malignant nodules in both hypoechoic nodules and isohyperechoic nodules (P<0.001 and P=0.004, respectively). MCTNs were associated with a higher malignancy risk in the hypoechoic nodule group (18.1%) than in the isohyperechoic nodule group (6.5%) (P<0.001). However, in both the hypoechoic and isohyperechoic nodule groups, the malignancy risks of MCTNs were similar to those of PCTNs (P=0.203 and P=0.092, respectively) and significantly lower than those of purely solid nodules (all P<0.001).
Malignancy Risk of Thyroid Nodules According to Composition and the Presence of Suspicious US Features
Table 4 presents the frequency and malignancy risk of thyroid nodules according to their composition and the presence of suspicious US features. MCTNs constituted 16.0% (242/1,514) of the group of nodules with suspicious US features and 24.9% (1,017/4,087) of the group of nodules without suspicious US features. MCTNs were more prevalent among benign nodules than among malignant nodules, both in the group of nodules with suspicious US features and in the group of nodules without suspicious US features (all P<0.001). MCTNs were associated with a higher malignancy risk in nodules with suspicious US features (20.7%) than in those without suspicious US features (6.0%) (P<0.001). However, in both nodules with and without suspicious US features, the malignancy risks of MCTNs were similar to those of PCTNs (P=0.272 and P=0.118, respectively) and significantly lower than those of purely solid nodules (all P<0.001).
Malignancy Risk of Thyroid Nodules According to Composition and Nodule Size
Purely solid nodules showed a higher malignancy risk in small nodules (Ōēż2 cm) than in large nodules (>2 cm) (P<0.001). In comparison, MCTNs and PCTNs did not show different malignancy risks according to nodule size (P=0.074 and P=0.141, respectively). In both small (Ōēż2 cm) and large (>2 cm) nodules, the malignancy risks of MCTNs were similar to those of PCTNs (P=0.093 and P=0.056, respectively) and significantly lower than those of purely solid nodules (all P<0.001) (Table 5).
Discussion
This multicenter study investigated the malignancy risk of thyroid nodules with minimal cystic changes. The distribution of purely solid nodules, MCTNs, and PCTNs was 3,041 (54.3%), 1,259 (22.5%), and 1,301 (23.2%), respectively. The overall malignancy risk of MCTNs was 8.8%, which was significantly lower than that of purely solid nodules (29.5%) (P<0.001). The overall risk of malignancy associated with MCTNs was 8.8%, which was higher than the previously reported result of 3.3%. A previous study [9] reported that the malignancy risk associated with purely solid nodules, MCTNs, and PCTNs was 14.8% (108/730), 3.3% (2/61), and 3.3% (7/209), respectively, with MCTNs showing the same malignancy risk as PCTNs. This difference might be due to the low prevalence of MCTNs (6.1%), few cases of hypoechoic MCTNs (n=9) and MCTNs with suspicious US features (n=6) in the previous study. In this study, MCTNs were more prevalent (22.5%) and there were many cases of hypoechoic MCTNs (n=249) and MCTNs with suspicious US features (n=242). The malignancy risks associated with hypoechoic MCTNs (18.1%) and MCTNs with suspicious US features (20.7%) were higher than those of isohyperechoic MCTNs (6.5%) and MCTNs without suspicious US features (6.0%), which might explain why the overall malignancy risk of MCTNs was higher in the present study than in the previous one [9].
Therefore, it seems appropriate to define solid nodules as purely solid nodules without obvious cystic components in the US lexicon, as this definition enables more accurate risk stratification and higher interobserver agreement. First, the malignancy risk of MCTNs was significantly lower than that of purely solid nodules. Second, the malignancy risk of MCTNs was similar to that of PCTNs in all subgroups categorized according to echogenicity or presence of suspicious US features. Although the overall malignancy risk was slightly higher in MCTNs than PCTNs, the malignancy risk estimated by US features is not based on a single US predictor, but rather a combination of US features [5,11-13].
Finally, a quantitative analysis of the cystic portion may not be accurate because solid nodules present as a continuum [6]. Estimating the cystic portion as <10% or <5% in a nodule is highly subjective, and high interobserver agreement might not be achievable [6,7]. Thus, defining solid nodules as purely solid nodules may help increase the interobserver agreement for solid composition. Moreover, in EU-TIRADS and ACR-TIRADS, minimally cystic nodules are classified as solid, so classifying minimally cystic nodules as partially cystic nodules would be expected to increase the accuracy of the RSS for thyroid nodules and reduce the unnecessary biopsy rate.
Previous investigators reported that most malignant thyroid tumors were solid (81.6%ŌĆō93%) [5,14-17], and the malignancy risk of solid nodules was higher (24.1%ŌĆō34.7%) than that of PCTNs (3.3%ŌĆō7.1%) [12-15]. This study showed similar results, as most of the malignant thyroid tumors were purely solid (82.4%), and solid tumors were associated with higher malignancy risk (29.5%) than PCTNs (6.2%) or MCTNs (8.8%). Accurately determining the presence of minimally cystic changes can be difficult in cases that include complicated cysts with hemorrhage or thick colloid materials, as well as in cases of fibrosis with marked hypoechogenicity [9,17]. In this study, nodules without obvious anechoic cystic change were categorized as purely solid nodules to enhance interobserver agreement.
This study has several limitations. First, cases without a final diagnosis or inconclusive biopsy results were excluded, which may have resulted in selection bias. Second, the retrospective assessment of static sonograms inherently limited the accuracy of the US interpretation for minimally cystic changes. Third, US features were described by different radiologists, resulting in interobserver variability; however, interobserver variability was not investigated in the present study.
The malignancy risk of MCTNs was low (8.8%) and significantly lower than that of purely solid nodules (29.5%). The risk of malignancy associated with MCTNs was similar to that of PCTNs, regardless of echogenicity or the presence of suspicious US features. Therefore, MCTNs could be categorized as PCTNs rather than as solid nodules to increase the accuracy of the risk stratification system for thyroid nodules.

 Download Citation
Download Citation PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Full text via PMC
Full text via PMC



