Impact of variations in fatty liver on sonographic detection of focal hepatic lesions originally identified by CT
Article information

Abstract
Purpose:
The aim of this study was to investigate the influence of variations in fatty liver on the ultrasonographic detection of focal liver lesions.
Methods:
A total of 229 patients with varying degrees of fatty liver and focal liver lesions and 200 patients with focal liver lesions but no fatty liver were randomly selected for inclusion in groups I and II, respectively. Findings of focal liver lesions identified on computed tomography were taken as the reference, and findings on ultrasonography were compared with them.
Results:
The number of focal liver lesions in groups I and II were 501 and 413, respectively. The ultrasonographic detection rates of focal liver lesions in groups I and II were 86.8% (435/501) and 94.2% (389/413), respectively. Comparison of the detection of the focal lesions between patients with and without fatty liver or different grades of fatty liver were as follows: mild fatty liver (162/177) vs. liver without fat infiltration (389/413) (P=0.277); mild fatty liver (162/177) vs. moderate fatty liver (190/212) (P=0.604); mild fatty liver (162/177) vs. severe fatty liver (83/112) (P<0.001); moderate fatty liver (190/212) vs. liver without fat infiltration (389/413) (P=0.051); moderate fatty liver (190/212) vs. severe fatty liver (83/112) (P<0.001); severe fatty liver (83/112) vs. liver without fat infiltration (389/413) (P<0.001); and fatty liver (435/501) vs. liver without fat infiltration (389/413) (P<0.001).
Conclusion:
Mild and moderate fatty liver are not significantly associated with the visualization of the lesion, while severe fatty liver usually impairs the detection of focal lesions in the liver. If a patient with severe fatty liver is suspected to have a liver tumor, ultrasonography should only be chosen cautiously in case of a missed diagnosis.
Introduction
Ultrasonography (US) and computed tomography (CT) are widely used for liver focal lesion screening, follow-up, or further evaluation. Together with magnetic resonance imaging (MRI), they play an important role in current clinical medicine. US examination is often the first-line modality for liver evaluation, and findings of US involve subsequent management in asymptomatic cases. A primary aim of US examination is to determine whether there is a space-occupying lesion or not, regardless of its nature. However, the effect of US evaluation of the liver is subject to several factors, such as the operator’s experience, the interference of gas, obesity, cirrhosis, fatty liver, and iron deposition [1-7]. Focal lesions may frequently be concurrent with fatty liver, for fatty liver (including non-alcohol fatty liver disease and liver fat infiltration from other causes) is common in the general population [8-10]. The presence of fatty liver may affect US imaging to some extent because focal lesions in fatty liver often show different features on imaging than those in a liver without fat infiltration [3,4,7,8], which sometimes results in the downgrading of a US diagnosis [4,7] but may not always impair visualization of tumors in the liver [3]. To our knowledge, no investigation has been conducted on the impact of different degrees of fatty liver on the US detection rate of focal liver lesions. The purpose of this study was to investigate the relationship of different degrees of fatty liver on the US detection of focal liver lesions.
Materials and Methods
Design, Setting, and Subject Selection
The Institutional Review Board of our affiliation approved this study and informed consent was waived due to the retrospective study design.
A study on the US detection rate of focal liver lesions in fatty liver was conducted from January 2010 through December 2014 in our hospital. Thirty thousand four hundred and twelve patients underwent US; among them 68 patients underwent unenhanced abdominal CT or combined chest and abdominal unenhanced CT; 195 patients underwent enhanced abdominal CT or combined chest and abdominal CT without precontrast CT; 2,027 patients underwent abdominal CT/enhanced CT or combined chest and abdominal CT/enhanced CT. Among the 2,027 patients who underwent both precontrast and contrast-enhanced CT, 1,839 patients were found with liver focal lesions. In the end, 1,241 patients with liver focal lesions were included in the study population, while 598 patients with glycogen storage disease, splenectomy, hepatic iron deposition, large lesions of diameter more than 9.0 cm and tiny lesions of diameter less than 0.5 cm were excluded; in addition, patients with more than 5 lesions in the liver were excluded due to the difficulty of accurately counting the number of lesions or absence of a concrete number in the records. The patients with focal liver lesions along with different degrees of fatty liver were categorized into groups with severe, moderate, and mild fatty liver. At first, 56 cases of severe and 92 cases of moderate fatty liver were all enrolled as group I; then 81 more cases of mild fatty liver were added to group I by selection with reference to a randomized table from the 308 cases of mild fatty liver. A subset of the patients with focal liver lesions but without fatty liver were selected with reference to a randomized table to be part of group II. In this way, 229 of 456 patients with fatty liver and focal liver lesions (134 males, 95 females; mean age, 36 years; range, 13 to 78 years) were selected as group I, and 200 of 785 patients with focal liver lesions and without fatty liver (119 males, 81 females; mean age, 33 years; range, 11 to 86 years) were selected as group II. Fig. 1 illustrates the flow chart of the study population and sample selection.
A flow chart of study population selection.
CT, computed tomography.
All procedures followed were in accordance with the ethical standards of the responsible committees on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008.
US Study
The US imaging study was performed by a sonologist (S.W.) with 15 years of experience, using an Aloka ProSound α 10 (Aloka Co. Ltd., Mitaka, Tokyo, Japan) and Mindray DC-8 (Mindray Medical International Ltd., Senzheng, China), with 5- to 2-MHz convex transducers.
CT Study
The CT scans were performed using 64-MDCT (LightSpeed VCT, GE Healthcare, Milwaukee, WI, USA) scanners. For the contrast-enhanced portions of the examinations, the patients received approximately 80-130 mL of iohexol (300 mgI/mL; Yangtze River Pharmaceutical Co. Ltd., Jiangsu, China) or intravenous iohexol (Omnipaque 300, GE Healthcare) or iodixanol (Visipaque 320, GE Healthcare) intravenously by means of a mechanical power injector (Stellant Injector System, Medrad Inc., Warrendale, PA, USA), administered at a rate of 3-4 mL/sec, followed by a 15- to 20-mL saline flush. The standard protocol for triphasic CT consisted of an unenhanced, arterial phase with a scanning delay of 30-40 seconds, and a portal venous phase with a scanning delay of 60-80 seconds.
Interpretation of the Images
The reference criterion for the diagnosis of fatty liver was the liver attenuation on the unenhanced CT. Hounsfield unit attenuation values of the liver and spleen were obtained through circular regions of interest representing the parenchyma on the unenhanced CT by a radiologist (R.T.), taking care to avoid visible vessels, bile ducts, focal lesions, calcifications, focal changes of fatty liver or fatty sparing, and the surface margins. The regions of interest were located in the right hepatic lobe and left hepatic lobe. The average of these two regions of attenuation was then obtained. The degree of the fatty liver was graded according to the criteria based on the ratio of the CT values of liver and spleen (L/S) proposed by Zeng et al. [11] in which 0.7<L/S ratio<1.0, 0.5<L/S ratio≤0.7, and L/S ratio≤0.5 corresponded to mild, moderate, and severe fat content categories, respectively.
Taking the findings on CT as reference, the presence or absence of focal liver lesions was determined, findings on US were compared, and several characteristics of the focal lesions were evaluated.
Statistical Analysis
The continuous variables included the size of the focal liver lesions, age of the patients, etc.; the discrete variables included the US detection rate of focal liver lesions in patients with and without fatty liver. The continuous variables were expressed as mean±standard deviation, while variables of different groups were compared using the independent samples t test. The non-continuous variables were analyzed using the chi-squared test. The statistical analyses were performed using IBM SPSS ver. 20 (IBM Co., Armonk, NY, USA). A P-value of less than 0.05 was considered to indicate a statistically significant difference.
Results
The number of patients with and without fatty liver, fatty liver grades, and lesions visible and invisible on US are listed in Table 1. The pathologic nature of the focal liver lesions based on histopathology (if available) and presumed diagnosis included cavernous hemangioma, 241; simple cyst, 107; metastatic tumor, 193; focal nodular hyperplasia, 5; adenoma, 2; hepatocellular carcinoma, 113; cholangiocarcinoma, 4; inflammatory pseudotumor, 5; solitary necrotic nodule, 2; and undetermined lesions, 242. The number of focal liver lesions in groups I and II were 501 and 413, respectively. The US detection rates of focal liver lesions in patients with and without fatty liver were 86.8% (435/501) and 94.2% (389/413), respectively (P<0.001).
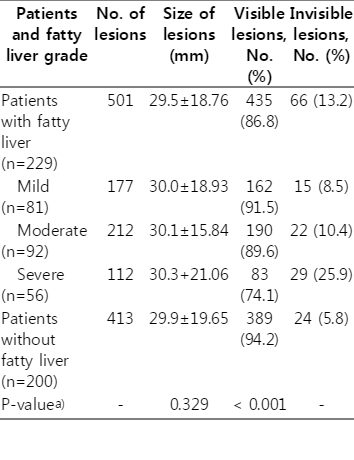
Number of patients by presence and extent of fatty liver, and lesions visible and invisible on ultrasonography
If a patient had several lesions, only the largest lesion was selected as representative for calculation of the mean size in a group. The size of focal liver lesions in group I ranged from 8 to 85 mm (29.5±18.76 mm), and the size of focal liver lesions in group II ranged from 7 to 87 mm (29.9±19.65 mm); the two groups showed no significant difference in size (P=0.329). In group I, 66 lesions (9-52 mm, 20.2±9.85 mm) were invisible on US (66/501), 24 lesions (9-53 mm, 21.3±12.5 mm) in group II were invisible on US (24/413), and there was no significant difference between the two groups in terms of lesion size (P=0.069). The comparison between patients with and without fatty liver or different grades of fatty liver showed the following with regard to the detection of focal lesions: mild fatty liver (162/177) vs. liver without fat infiltration (389/413) (P=0.277); mild fatty liver (162/177) vs. moderate fatty liver (190/212) (P=0.604); mild fatty liver (162/177) vs. severe fatty liver (83/112) (P<0.001); moderate fatty liver (190/212) vs. liver without fat infiltration (389/413) (P=0.051); moderate fatty liver (190/212) vs. severe fatty liver (83/112) (P<0.001); severe fatty liver (83/112) vs. liver without fat infiltration (389/413) (P<0.001); and fatty liver (435/501) vs. liver without fat infiltration (389/413) (P<0.001). Fig. 2 illustrates attenuation measurement on computed tomography image and Figs. 3-5 illustrate the focal liver lesions detected by CT and US.
Example of region of interest (ROI) placement for attenuation measurement on an unenhanced axial computed tomography image.
Three ROIs are placed in the liver at the level of the hepatic portal, and one is placed in the middle portion of the spleen. The liver measured 13 HU and the spleen measured 49 HU, consistent with fatty infiltration of the liver. HU, Hounsfield unit.
A 37-year-old man with two hepatic hemangiomas (16-21 mm in diameter) and three cysts (15-22 mm in diameter), and whose liver does not have fat infiltration.
A. At ultrasonography examination, only liver cysts are detected (arrows), and no hemangioma is visualized. B. Axial contrast-enhanced computed tomography image obtained at the arterial phase shows two low-density lesions enhancing centripetally and slowly, while the three lower lesions were found to lack enhancement (not shown). The image obtained in the portal venous phase shows two low-density lesions enhancing centripetally (arrows), but the three lower lesions still did not have enhancement. The results suggest that the two low density lesions are hepatic hemangiomas, and the three unenhanced lesions are cysts.
A 54-year-old man with hepatocellular carcinoma (40 mm in diameter), and whose liver does not have fat infiltration, but with liver parenchyma that is coarse due to fibrosis.
A. At ultrasonography examination, no liver focal lesion is visualized. B. An axial unenhanced computed tomography (CT) image shows the presence of a liver focal lesion (arrow). The CT value of the liver is 63 HU and spleen is 55 HU, which is consistent with liver without fatty infiltration. C. Axial contrast-enhanced CT image obtained at the arterial phase shows rapid enhancement of the lesion (arrow). D. Axial contrast-enhanced CT image obtained in the portal venous phase shows the quick “washout effect” of the lesion (arrow). The results indicate that the focal lesion is hepatocellular carcinoma. HU, Hounsfield unit.
A 29-year-old man with severe fatty liver and focal liver lesion (26 mm in diameter).
A. Axial unenhanced computed tomography (CT) image shows the lesion presenting slightly lower density (arrow) relative to the abutting parenchyma. The CT value of the liver is 18 HU and that of the spleen is 53 HU, which is consistent with fatty infiltration of the liver. B. Axial image obtained in the arterial phase of enhanced CT shows the lesion has no enhancement (arrow). C. Axial image obtained in portal venous phase of enhanced CT shows the lesion has no enhancement (arrow). The results suggest the lesion is a cyst. D. Image in the transverse plane obtained by ultrasonography shows high echogenicity of the liver parenchyma and substantial attenuation; the gallbladder (arrow) is partially obscured, and the diaphragm and liver veins are almost invisible. No focal lesion is visible in the liver. HU, Hounsfield unit.
Discussion
For the focal lesion assessment in the fatty liver, many reports have noted the difficulty of image interpretation due to the change in the echo pattern of the focal lesions on a fatty background [4,7,8,12]. However, the performance of US in the detection of focal liver lesions in fatty liver has not yet been thoroughly addressed. In the present study, the detection rate of focal liver lesions on US in patients with severe fatty liver was significantly lower than in other patients.
A study by van Vledder et al. [3] showed that the quality of US is poorer overall in the presence of fatty liver; some hypoechoic colorectal liver metastatic cancers become more conspicuous in fatty liver, and some hyperechoic or isoechoic lesions without accompanying fatty liver become less conspicuous in fatty liver. This indicates that some focal lesions become easier to visualize in the presence of fatty liver, but others are the opposite. The US visualization of a focal lesion might depend on both the intrinsic echogenicity of the lesion and the contrast between the lesion and the surrounding parenchyma, in conjunction with the size, location, and depth of the lesion. Apart from the influence of the contrast in resolution between the focal lesion and the surrounding parenchyma with greater echogenicity, the presence of fatty liver would negatively affect the ultrasound beam penetration, resulting in a compromise of focal lesion detection. It is well known that hepatic veins appear thin or obscure in moderate and severe fatty liver. The reason for this phenomenon is not that the hepatic veins become thin or disappear, but the impact of the presence of fatty liver. With severe fatty liver, even the gallbladder wall becomes blurry when it is scanned axially from the intercostal region; yet, when scanned obliquely from the subcostal region, which keeps away the thick liver parenchyma, it appears distinct. Our study results seemed to be consistent with the fact that severe fat infiltration in the liver is known to cause acoustic attenuation and to obscure the visualization of the intrahepatic structures and focal lesions.
Teefey et al. [1] reported that small size was the most common cause of a missed diagnosis of focal liver lesion in US, CT, or MRI. In the present study, the detectability of the lesions varied significantly between the cases with fatty liver and those without fat infiltration, but the sizes of the invisible lesions in the two groups were not significantly different from each other. Moreover, the lesions invisible in our study were not the smallest ones or all smaller entities. This indicated that lesion size is not the dominant factor affecting the visualization of focal liver lesions in the presence of fat infiltration. In clinical practice, some tiny punctate calcifications in the liver can be detected without effort due to their high echogenicity, which has much higher contrast to the liver parenchyma than that of other lesions; furthermore, if any lesion is located in the surface of the liver, it should also be readily visible regardless of the lesion size. In terms of the relationship to fatty liver, lesion size should not have a notable effect on the detection rate of focal liver lesions.
The potential limitations of this study include the following: (1) Only those lesions frequently encountered in clinical practice, but not the less common larger and smaller lesions, were included, which may have resulted in sampling bias. On the other hand, the samples were acquired from groups of patients with and without fatty liver in the same way, and no significant difference in the lesion size was found between the two groups; therefore, the sampling bias is negligible. (2) No stratified analysis according to the size range of the lesions was performed, which may have affected the accuracy of analysis of the relationship to fatty liver. However, the results of this study show that the size of lesions invisible in the two groups was not significantly different, which indicates that the absence of size stratification had little effect on the analysis. (3) The correlation of histological findings was limited, and no data analysis was performed that distinguished between benign and malignant lesions. However, cystic lesions are easier to detect in the liver than solid lesions in general. In this study, the samples were selected by randomization, so bias caused by the lesion’s pathology would have been limited. (4) No echoic texture analysis was performed for individual lesions, which may have affected the analysis in individual cases. However, the sample of this study was relatively large, and the impact of echoic texture is trivial.
In conclusion, the results of our study showed that a fatty liver background did not always influence the detection of focal lesions in the liver; specifically, mild and moderate fatty liver did not significantly affect the visualization of lesions, while severe fatty liver impaired the detection of focal lesions in the liver. Therefore, clinicians should be aware that if a patient with mild fatty liver is suspected of having a liver tumor, noninvasive US can be used primarily, but if a patient with severe fatty liver is suspected to have a liver tumor, US should only be used cautiously, given the potential for a missed diagnosis.
Notes
No potential conflict of interest relevant to this article was reported.
Acknowledgements
The authors would like to express their gratitude to the sonologists, Li Huang, Ying Wan, Shibin Lin, Enhai Zheng, Chuan Fu, Kailiang Chen, and Yanyan Zhao for their assistance.